Palpitations: a common symptom that could be serious
Articles in this section use cases to illustrate the emergency management of patients presenting in general practice with cardiac problems. They are inspired by, but not based on, real patient situations.
Dr JP is particularly aware of the palpitations at night and when lying on his left side (as the heart moves closer to the chest wall). He has identified runs of bigeminy (a continuous alternation of long and short heart beats) and trigeminy (a ventricular premature beat after two normal beats) by palpation of his heart and peripheral pulse. There seems to be a background sinus rhythm.
At first, Dr JP thought the palpitations were related to the three to four cups of coffee he was drinking each day, his beta-agonist asthma inhaler or myocarditis from a mild viral infection. As he eliminated each of these, there was no change to his symptoms. He became concerned due to his health history.
Dr JP is a nonsmoker and does not have diabetes; however, he does have a history of vascular disease. Seventeen years ago, he needed an urgent carotid endarterectomy due to an almost occluded artery. He had quadruple bypass coronary graft surgery 10 years ago and three cardiac stents implanted five years ago. Two years ago, a stent was implanted in his left femoral artery and one year ago two stents were implanted in his right femoral artery.
Dr JP has a small-calibre atherosclerotic arterial system. His risk factors are hypertension (treated with candesartan 8 mg daily) and high cholesterol levels (treated with a strict diet and low-dose statins, although these were not well tolerated as he experienced major muscle symptoms). He also takes cholestyramine 8 g daily in orange juice, clopidogrel 75 mg daily, aspirin 100 mg daily and allopurinol 100 mg daily.
He had not had any myocardial infarction or stroke. His parents both lived to 80 years of age, his father died from an aortic aneurysm and his mother died with vascular multi-infarct dementia.
What is the next step?
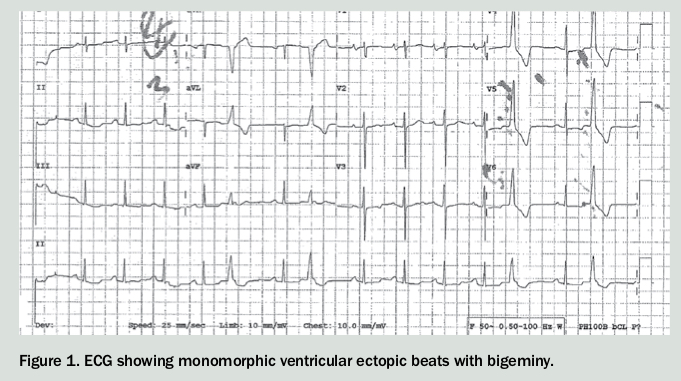
Dr JP experiences palpitations during the consultation. His blood pressure is 155/90 mmHg and his pulse rate is 96 beats per minute (bpm). You perform an ECG (Figure 1).
{kind=link}
His ECG shows monomorphic ventricular ectopic beats with bigeminy. There is no short PR interval. There is a normal QT interval and no signs of previous infarct.
At the time of the ECG, Dr JP has symptomatic palpitations. However, he has no other symptoms, such as light headedness, presyncope, chest pain or shortness of breath, and therefore no predictors of serious arrhythmias such as ventricular tachycardia (VT).1
What are the differential diagnoses?
Palpitations are a common reason for patients to seek medical care. The main aetiologies associated with palpitations are:2
- cardiac causes
- psychiatric causes
– panic attacks
– anxiety disorder
– depression
- other causes
– medication-induced, e.g. beta agonists, anticholinergic agents
– thyrotoxicosis
– caffeine consumption
– cocaine use
– amphetamine use
– anaemia
Independent predictors of a cardiac cause for palpitations are:2
- male sex
- irregular heart beat
- history of heart disease
- duration of palpitations of more than five minutes.
Given Dr JP’s history and your findings, you consult his cardiologist who agrees to see him that afternoon. At the consultation a repeat ECG is very similar to the first and laboratory tests performed at your practice are unremarkable.
What further investigations are required?
An echocardiogram (to assess the left ventricular function) and a Holter monitor are ordered. The cardiologist discusses the possible results with Dr JP, including the fact that most palpitations and ectopic beats are benign and that bigeminy and trigeminy have no known prognostic significance. He clarifies that the main predictors of serious arrhythmias include structural cardiac damage and older age.
Three days later Dr JP has the Holter monitor fitted and the echocardiogram follows. He returns to your surgery for the results. The 24-hour computer read out from the Holter monitor is 9000 ectopic beats (more than 10,000 is considered significant). It also shows 15 beats of nonsustained monomorphic VT at a rate of 180 bpm. As per protocol, his cardiologist is rung. Because of the known history of vascular disease urgent cardiac catheterisation is performed the next day to exclude a coronary occlusion.
What does cardiac catheterisation show and what is the next step?
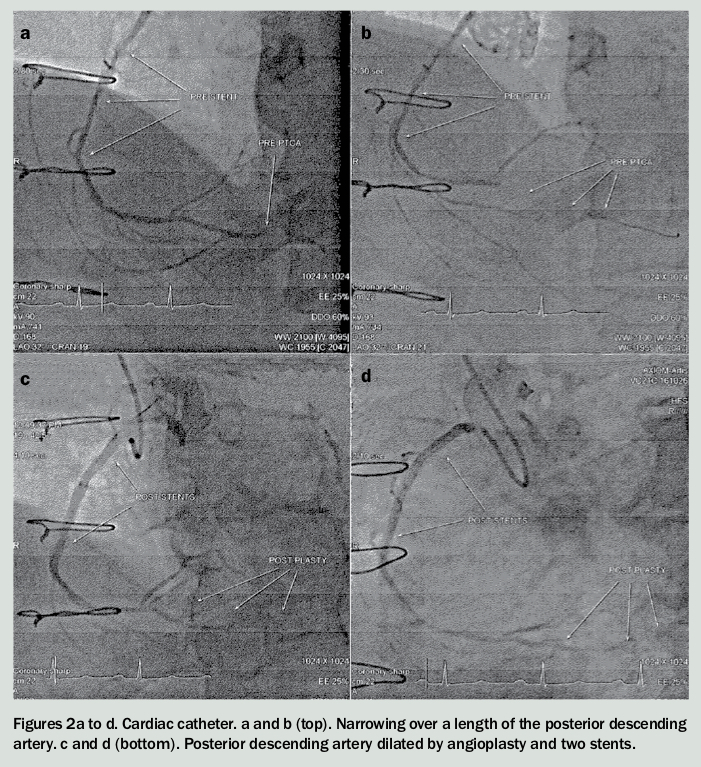
Cardiac catheterisation shows no acute occlusion. However, increased pathology – narrowing over a length of the posterior descending artery – is found, which would be difficult to treat (Figures 2a and b).
{kind=link}
Dr JP is referred to an electrophysiologist who arranges an electrophysiology study which shows the ectopy is from the myocardium supplied by the posterior descending artery. The electrophysiologist explains that the significance of nonsustained VT is poorly understood but that it is common. It is often an incidental finding on cardiac monitoring although there is no clear prognostic information available about cardiac mortality.1
Outcome: Discussion between the cardiologists and with Dr JP resulted in a further cardiac catheterisation being performed two weeks later. The posterior descending artery is dilated by extensive angioplasty and two stents are inserted. The result is good flow and new flow in opened up branches (Figures 2c and d).
His antihypertensive medication is changed to diltiazem 180 mg daily.
Dr JP reports no more runs of bigeminy or trigeminy. His resting heart rate slowed by 10 to 15 bpm but still beats ectopically occasionally, as would be expected, and he is being followed up by his cardiologists. CT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.