Palpitations
Articles in this section are inspired by, but not based on, real cases to illustrate the importance of knowledge about ECGs in relation to clinical situations in general practice. Management is not discussed in detail.
- In adults, on an ECG, T waves are normally upright in leads I, II, and V3 to V6, inverted in aVR and sometimes V1, and variable in leads III, aVL, aVF and V2.
- New or deep symmetrical T wave inversions are abnormal, particularly in the lateral (I, aVL, V5, V6) or inferior (II, aVF) leads, and may indicate ischaemia or cardiomyopathy. Other potential causes include right bundle branch block, pulmonary embolism or incorrect limb lead placement.
- The differential diagnoses for palpitations that occur at rest include sinus tachycardias, supraventricular tachycardias, atrioventricular nodal re-entry tachycardias, Wolff–Parkinson–White syndrome or ventricular tachycardias.
- Management involves appropriate investigations such as Holter monitoring, blood tests and echocardiography, with treatment tailored to the underlying cause.
You do not know Stefan, a fit-looking 42-year-old, English-speaking Romanian man who has been living in Australia for several years. He has attended your practice a few times, but not recently. He is very stressed and comes to see you because he has been experiencing heart palpitations over the past week, associated with sharp pains in his left chest that last for seconds, are worse with movement of his left arm and are accompanied by pain in his left elbow. He is worried about his heart. He takes no medications and has no significant past medical history. He is a nonsmoker.
Stefan tells you that by palpitations, he means his heart is beating forcefully and fast. He has not measured the rate, but thinks it is over 100 beats per minute and regular. He feels stressed and nonspecifically unwell at present, and feels worse because of family problems back in Romania. He has had mild nausea lately, and has had no faintness or sweating with the palpitations. These episodes tend to occur in the evening and overnight when he is not working, and can last for hours. He is not sleeping well and feels the palpitations may be disturbing his sleep. They do not start suddenly, but he has had some success reducing them to what he considers to be a ‘fast normal rate’ with relaxation techniques.
He works as a builder and is self-employed, but has stopped working because he is worried he may die from a heart condition. He does not have a family history of any heart condition or sudden death, and he says his cholesterol and blood pressure have always been normal. He has no psychiatric history.
On examination, Stefan’s blood pressure is 138/90 mmHg and his pulse is 67 beats per minute and regular. His heart sounds are normal, his apex is normal and he has no heart murmurs or bruits. His chest is clear and palpation of the chest wall is nontender. He looks stressed. His left elbow looks normal but is tender around the lateral epicondylar region.
It is important to take him seriously and not assume this is anxiety. You therefore organise an ECG (Figure), 24-hour Holter monitor, full blood count, thyroid function tests, serum troponin (to exclude myocarditis), iron studies, C-reactive protein, liver and kidney function tests, and measurement of nonfasting blood glucose, cholesterol, triglycerides, and high- and low-density lipoprotein levels.

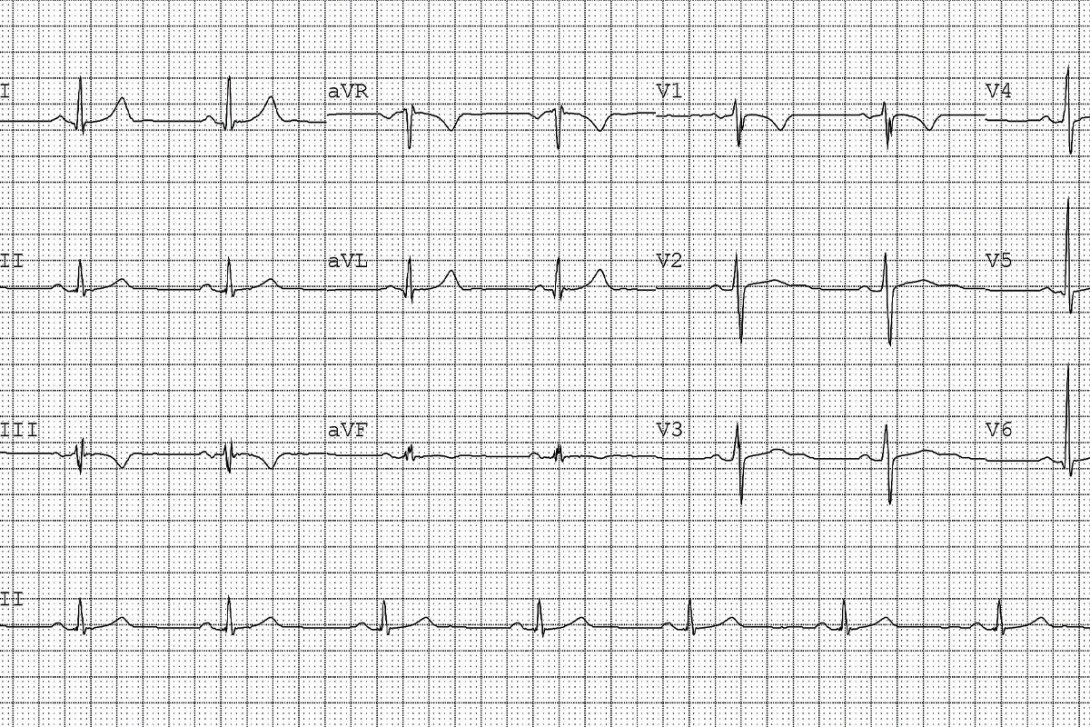
Q1. What does the ECG show?
The ECG shows a heart rate of 51 beats per minute in sinus rhythm. The corrected QT interval is 417 ms. He has T wave inversion in leads III and V1.
Q2. What are T waves?
The T wave represents ventricular repolarisation on the ECG. It is normally upright in leads I, II and V3 to V6, and is normally inverted in aVR and sometimes V1.
T waves are variable, but often upright, in leads III, aVL, aVF and V2. They are usually 1 to 5 mm in amplitude in leads I, II and III, and 2 to 10 mm in amplitude in leads V1 to V6. Their duration is not normally measured. The duration of the T wave contributes substantially to the QT interval (which also includes the QRS duration and ST segment).
T wave inversion in leads V1 to V3 is normal in children. Biphasic T waves may be seen in myocardial ischaemia and hypokalaemia.
Q3. Is this ECG normal?
It can certainly be a normal variant to have T wave inversion in leads III and V1. T waves may also continue as a persistent juvenile T wave pattern in some adults as a normal variation in leads V1 to V3. It would be unlikely that Stefan has a cardiomyopathy as the cause of the T wave inversion in leads III and V1, as there are no other concerning ECG features such as T wave inversion in leads I, II or V3 to V6.
There is a mild bradycardia present in this ECG that is likely due to Stefan’s physical fitness. A normal resting heart rate is 60 to 100 beats per minute, depending on factors such as stress and aerobic fitness. Overall, this ECG is normal.
Q4. When are T wave inversions in lead III not normal?
New T wave inversions are not normal and neither are deep (more than 3 mm in lead III) symmetrical T waves. It is also not normal to have T wave inversion in other leads, especially the lateral leads (I, aVL, V5, V6) and inferior leads (II, aVF). If the T wave inversion is associated with ST abnormalities or significant Q waves, the ECG may represent cardiac ischaemia or cardiomyopathy. Incorrect limb lead positioning may result in spurious T wave inversion in lead III.
Right bundle branch block can produce deeper T waves in lead III, but this block is not present on this ECG. There is no RSR’ pattern (M-shaped) QRS complex in V1 and V2, no wide slurring of the S wave in the lateral leads (I, aVL and V5 to V6) and the QRS duration is under 120 ms.
Pulmonary embolism is another cause of T wave inversion in the inferior leads (II, III and aVF) and right precordial leads (V1 to V3), but this diagnosis is unlikely given the clinical history. Other causes of acute right heart strain (e.g. chronic obstructive pulmonary disease, pulmonary hypertension) are also clinically unlikely given Stefan’s general fitness and him being a nonsmoker.
None of the pathological features described above are present in this ECG and the T wave inversion has reassuringly been documented on his previous ECG.
Q5. What are the differential diagnoses of regular palpitations at rest?
Sinus tachycardias may arise from stress, fever, hypoglycaemia, dehydration, medications (stimulants such as beta agonists, attention deficit hyperactivity disorder medications, phentermine and caffeine, as well as drugs such as amphetamines and cocaine), drug withdrawal and hyperthyroidism. Or they may be ‘inappropriate’ – with none of the above triggers present, and therefore presumed to be due to a primary abnormality of sinus node function.
Other tachycardias include supraventricular tachycardias (atrial tachycardia, atrial flutter), atrioventricular nodal re-entry tachycardias, Wolff–Parkinson–White syndrome (where an accessory electrical pathway connects the atria to the ventricles) and ventricular tachycardias (where heart rates can range from 120 to 300 beats per minute).
Outcome
The 24-hour Holter result was normal with a sinus rate of 50 to 120 beats per minute, with rare ventricular ectopics. No symptoms were recorded by Stefan when the Holter monitor was worn, and his blood tests came back normal. Stefan still felt there was a problem with his heart and so a cardiac echocardiogram was arranged, mainly to exclude an early cardiomyopathy or congenital abnormality such as an atrial septal defect.
This test showed normal left and right ventricular size, wall thickness and contractility, but there was a mildly dilated left atrium and a moderately dilated aortic root (47 mm), with a mildly dilated ascending aorta (39 mm). There was also trivial pulmonary and aortic regurgitation and otherwise normal valves.
Stefan was referred to a cardiologist who recommended further ambulatory monitoring (with longer Holter monitoring or with an event monitor) to achieve symptom–rhythm correlation. Given the combination of a dilated aortic root and left atrial dilatation, strict blood pressure control was recommended. He was advised to reduce salt in his diet and was started on a low-dose angiotensin receptor blocker. He will have ongoing follow up. He visited his GP for further review and was offered antidepressants or counselling to assist him in returning to work and managing his anxiety. CT
COMPETING INTERESTS: None.
Further reading
Burns E. T wave [Internet]. Life in the Fast Lane 2024. Available online at: https://litfl.com/t-wave-ecg-library/ (accessed September 2025).
Burns E, Buttner R. Right bundle branch block [Internet]. Life in the Fast Lane 2024. Available online at: https://litfl.com/right-bundle-branch-block-rbbb-ecg-library/ (accessed September 2025).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.