‘My heart is always going fast, Doctor’
Articles in this section are inspired by, but not based on, real cases to illustrate the importance of knowledge about ECGs in relation to clinical situations in general practice. Management is not discussed in detail.
- Atrial fibrillation (AF) is the most common pathological tachyarrhythmia and is characterised by an irregularly irregular rhythm, absent P waves and variable R-R intervals.
- Acute infection and sepsis are important reversible causes of both AF and sinus tachycardia, particularly in older people.
- Multiple atrial ectopics and short runs of atrial ectopics are associated with increased risks of AF and stroke, as well as increased mortality.
- Dilated atria, especially left atrial dilation, are an independent risk factor for AF.
- Sinus tachycardia may result from physiological stress, medications, metabolic disturbances or serious underlying pathology and should always be interpreted in clinical context.
Imelda is an 83-year-old woman with obesity who is incapacitated by osteoarthritis. She mobilises with a walker and has recently moved to the area of your practice; you have now met her a few times. She is brought in by her niece because she is feeling unwell. You note her breathing appears slightly more laboured than usual as she walks in. She says she has been more tired over the past day or so and her appetite is poor. She reports no other symptoms of relevance.
Imelda takes amlodipine 5 mg daily, aspirin 100 mg daily, bisoprolol 10 mg daily, alendronate/cholecalciferol 70 mg/140 microg weekly, methenamine hippurate 1 g twice daily, atorvastatin 80 mg daily, telmisartan 40 mg daily and oxycodone/naloxone 2.5 mg/1.25 mg twice daily. She has also been diagnosed with osteoporosis, hypertension and aortic sclerosis, and her last echocardiogram, performed a year ago, was consistent with heart failure with preserved ejection fraction. Her blood pressure at a previous visit was 135/85 mmHg and her pulse was 105 beats per minute and regular.
You begin by taking Imelda’s blood pressure. This is difficult to ascertain because the screen repeatedly reads ‘error’. You palpate her wrist while Imelda is sitting during repeat sphygmomanometry. You feel systolic beats at around 110 to 120 mmHg, variable in amplitude and irregularly irregular. You examine Imelda’s cardiorespiratory system. Her apex beat is irregularly irregular at a rate of 137 beats per minute and there is a midsystolic murmur consistent with aortic sclerosis. Her apex is otherwise normal. Her lungs sound clear and she is not short of breath at rest.
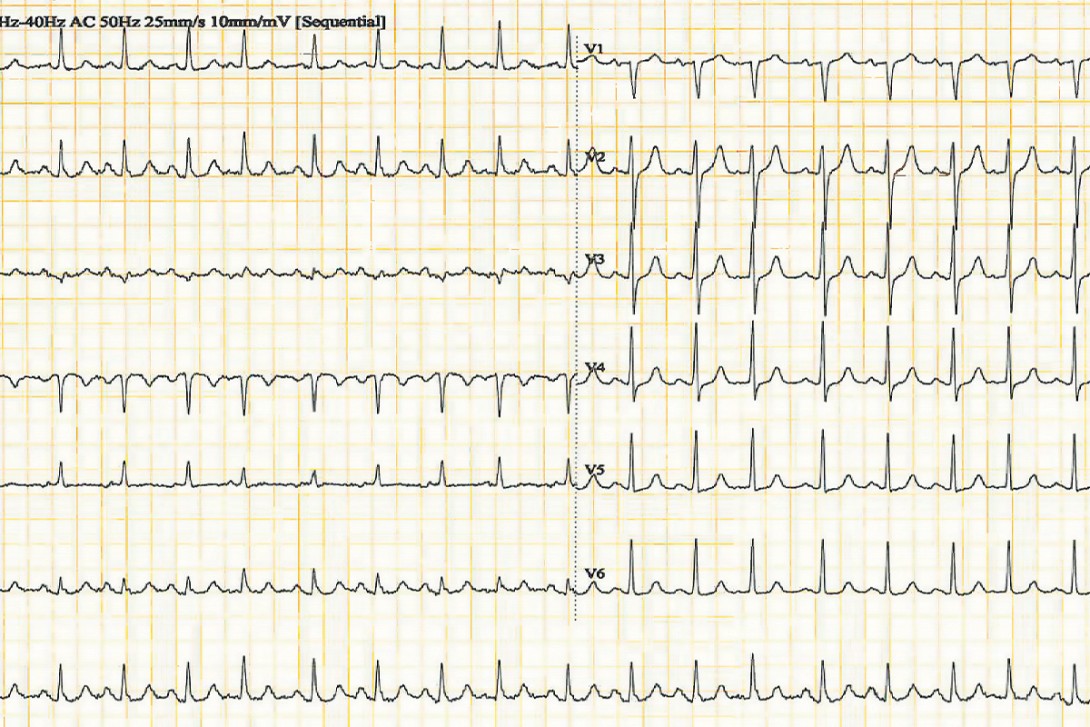
You arrange an urgent ECG in the surgery (Figure), but this takes 30 minutes to obtain. The nurse records Imelda’s temperature as 37.7°C measured aurally.

Q1. What does Imelda’s ECG show?
The ECG shows sinus tachycardia at 116 beats per minute with atrial premature beats.
Q2. What are you thinking and what should be the next step at this stage?
The issue is that Imelda feels unwell, is mildly febrile and has likely paroxysmal atrial fibrillation (AF) or frequent ectopy. These two findings may be connected, but the AF requires specialist review because this is a new finding.
You initially discuss Imelda’s case with the emergency department consultant at the local regional hospital, requesting monitoring for several hours. However, he is overwhelmed with work and says her cardiologist should deal with this. The cardiologist (who has met Imelda only once recently, when she was stable) insists that the emergency department monitor the patient, perform appropriate investigations and assess why she is feeling unwell.
You discuss hospital admission with Imelda on the basis that her pulse rate was very fast and irregular when you assessed her before the ECG, and is still faster than normal for her. You are concerned about her going home without a diagnosis or management of this possible intermittent tachyarrhythmia.
Imelda raises her eyes and says: ‘Oh no, not again. My pulse is always fast. It is always between 90 and 115 beats per minute.’ Her niece tells her to go to hospital. Imelda agrees, and you arrange an ambulance.
Q3. What is AF and what causes it?
AF is the most common pathological tachyarrhythmia.¹ It is caused by the atria contracting continuously and chaotically, resulting in irregular conduction of electrical impulses through the atrioventricular node. This produces R-R interval variability, absent P waves and an undulating baseline. The ventricular response may be slow (slow AF), normal or fast (rapid AF).
Common causes include acute ischaemic heart disease, valvular disease (especially mitral valve prolapse), serious acute infections, cardiac surgery, heart failure, hyperthyroidism, hypertensive heart disease, cardiomyopathy, myocarditis, pulmonary embolism, drug and alcohol intoxication, and severe metabolic derangements, particularly electrolyte abnormalities and anaemia. AF is also strongly associated with advanced age.
Beta agonists, such as salbutamol and salmeterol, have been associated with AF. AF may also occur spontaneously in the absence of structural heart disease or other precipitants.
Q4. What is the definition of sinus tachycardia and what are its causes?
Sinus tachycardia is a regular resting heart rate greater than 100 beats per minute in an adult.² The pulse rate of babies and children progressively reduces to this rate with increasing age. The ECG demonstrates regular P waves and QRS complexes.
Causes include increased circulating catecholamines (exercise, stress and emotional upset), recreational drugs (such as cocaine, amphetamine derivatives and nicotine), withdrawal of addictive substances, prescription medications (such as dexamphetamine and alpha-adrenergic agonists) and pathological causes, such as fever, sepsis, dehydration, haemorrhage, anaemia and shock. (A comprehensive list of medications and drugs that may cause sinus tachycardia, or withdrawal of which may cause sinus tachycardia, may be found in reference 2.) Cardiac causes include myocarditis, cardiac tamponade and acute coronary syndrome. Respiratory causes include hypoxia, restrictive and obstructive lung disease and pulmonary embolism. Hypoglycaemia and electrolyte disorders, including hypokalaemia, hypocalcaemia and hypomagnesaemia, may also result in sinus tachycardia.
Q5. What is the significance of multiple atrial ectopics (premature atrial complexes) or runs of atrial ectopics on an ECG or Holter monitor?
Multiple atrial ectopics are an independent risk factor for AF and stroke. Short runs of atrialectopics increase the risk of a patient developing AF or already having AF.³
Short runs of atrial ectopics and frequent atrial ectopics are also associated with increased mortality, particularly from ischaemic stroke, independently of a history of AF.³ In a meta-analysis, excessive atrial ectopy was defined as more than 30 ectopics per hour or any runs of more than 20 consecutive atrial ectopic beats on ambulatory ECG monitoring.³ These findings are therefore not considered benign, as was previously thought.
Q6. What is the significance of dilated atria on echocardiography with respect to AF?
The cause of AF at the cellular level is not fully understood. AF may arise from one or more abnormal foci within the atria or pulmonary veins, or chaotic multiple wavelet re-entry within the atria. Dilated atria, especially left atrial dilation, from any cause are a well-known risk factor for AF.
AF, either intermittent or chronic, results in increased atrial pressure during cardiac contraction. This contributes to electrical and structural remodelling over time, and recurrent or chronic AF can worsen these changes, causing a vicious cycle of increased atrial dilation and more frequent fibrillation.4
To emphasise, dilated atria, particularly the left atrium, are an independent risk factor for AF.4
Outcome
At the hospital, Imelda underwent two ECGs over two hours, a chest x-ray, serum troponin testing and routine blood tests. All results were stable. Later that day, Imelda developed a high fever and became confused. She was admitted with an acute urinary tract infection. A urine sample was taken and sent for culture. Further cardiac monitoring was not performed.
After discharge, Imelda’s cardiologist confirmed an unchanged echocardiogram, with a left ventricular ejection fraction of 55% and mild atrial dilation. In retrospect, the likely brief episode of AF and sinus tachycardia were considered secondary to sepsis, and anticoagulation or preventive therapy was not recommended because the episode had been brief and the precipitant was known.
This ECG clinic highlights the importance of considering acute infection as a cause in patients presenting with either sinus tachycardia or AF. Ongoing vigilance for recurrent AF is recommended and can be achieved with ambulatory monitoring, including Holter monitors, event monitors and smartwatches. If longer episodes of AF are detected, anticoagulation would be recommended to reduce the risk of stroke and other thromboembolic events. CT
COMPETING INTERESTS: None.
References
1. Burns E, Buttner R. Atrial fibrillation ECG library. Life in the Fast Lane; 2024. Available online at: https://litfl.com/atrial-fibrillation-ecg-library/ (accessed June 2026).
2. Henning A, Krawiec C. Sinus tachycardia. Treasure Island (FL): StatPearls Publishing; 2023. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK553128/ (accessed June 2026).
3. Meng L, Tsiaousis G, He J, et al. Excessive supraventricular ectopic activity and adverse cardiovascular outcomes: a systematic review and meta-analysis. Curr Atheroscler Rep 2020; 22(4): 14.
4. CardioSmart. Enlarged heart linked to atrial fibrillation. Washington, DC: American College of Cardiology; 2015. Available online at: https://www.cardiosmart.org/news/2015/8/enlarged-heart-linked-to-atrial-fibrillation (accessed June 2026).