Heart failure. Re-admissions are just the tip of the iceberg

Heart failure
Managing patients with heart failure presents a significant challenge for GPs. Hospitalisation will sometimes be necessary for stabilisation, despite optimal medical therapy and lifestyle measures.
- An admission with decompensated heart failure typically has a poor prognosis.
- There is scope for improvement in the management of these patients, both from an inpatient optimisation point of view and in the ambulatory setting.
- Achieving and maintaining euvolaemia is an essential aspect of preventing rehospitalisation and reducing the symptom burden of heart failure.
- Early follow up (within one week) with the patient’s GP is an effective means of reinforcing these measures and preventing repeat hospitalisations.
Case scenario
Mr JS, a 65-year-old man with diabetes, presented with exertional dyspnoea, orthopnoea and peripheral oedema and was admitted to hospital with a diagnosis of decompensated heart failure. His relevant past medical history was:
- ischaemic heart disease with percutaneous coronary intervention
- coronary artery bypass grafts after a non-ST-elevation myocardial infarction five years previously
- mild systolic impairment with moderate pulmonary hypertension and mild aortic stenosis
- obstructive sleep apnoea, which was untreated as the patient was unable to tolerate a mask
- type 2 diabetes for which the patient was insulin dependent
- macrovascular complications of coronary artery disease, peripheral vascular disease and ischaemic stroke
- microvascular complications of peripheral neuropathy and retinopathy
- mild cognitive impairment in the context of previous stroke and earlier traumatic brain injury.
Mr JS’s presentation occurred two days after he was discharged from a prolonged admission to hospital for treatment of an infected diabetic foot ulcer, with a resultant period in rehabilitation. After his discharge, Mr JS had difficulty accessing his prescription medications and therefore did not receive his regular diuretics.
The diagnosis of decompensated heart failure required a prolonged admission for Mr JS who received intravenous diuretics and inotropes to restore euvolaemia.
Mr JS represents an increasingly common group of patients with heart failure as one of multiple comorbidities. In this patient group, treatment of one condition impacts and interacts with the management of others.
The burden of heart failure hospitalisation
The Victorian Cardiac Outcome Registry (VCOR) conducts an annual Heart Failure Snapshot.1 In 2016, most patients admitted to hospital with heart failure were men (58%) with a median age of 76 years. The most common comorbidities, seen in our case scenario, are atrial fibrillation (54%), diabetes (47%), anaemia (36%), a history of angina (34%), chronic obstructive pulmonary disease (COPD; 31%) and moderate renal dysfunction (31%).
A patient admitted with decompensated heart failure typically has a poor prognosis. From the VCOR data, of those admitted with heart failure, there was an unadjusted 30-day mortality rate of 9.9%, which is comparable with international benchmarks. Significantly, there was a 21% all-cause readmission rate within 30 days of discharge. Accordingly, there is scope for improvement in the management of these patients, both from an inpatient optimisation point of view and in the ambulatory setting. GPs, heart failure nurses, cardiologists, general physicians and other allied healthcare professionals can have a major impact in the ambulatory setting on reducing rates of readmission.
Achieving and maintaining a euvolaemic fluid balance
Achieving and maintaining euvolaemia is an essential aspect of preventing rehospitalisation and reducing the symptom burden of heart failure. Lifestyle, dietary and pharmacological interventions are often instituted in the hospital setting, but ongoing education and management are typically required in the ambulatory setting. Early follow up (within one week) with the patient’s GP is an effective means of reinforcing these measures and preventing repeat hospitalisations. The following should be considered in the initial consultations.
Dietary and lifestyle measures
Dietary measures such as adherence to a low-sodium diet (less than 2g daily) and fluid restriction (1.5L daily) are important aspects of patient education and management following an admission for heart failure. Encouraging alcohol reduction or abstinence is also recommended.
Monitoring fluid status
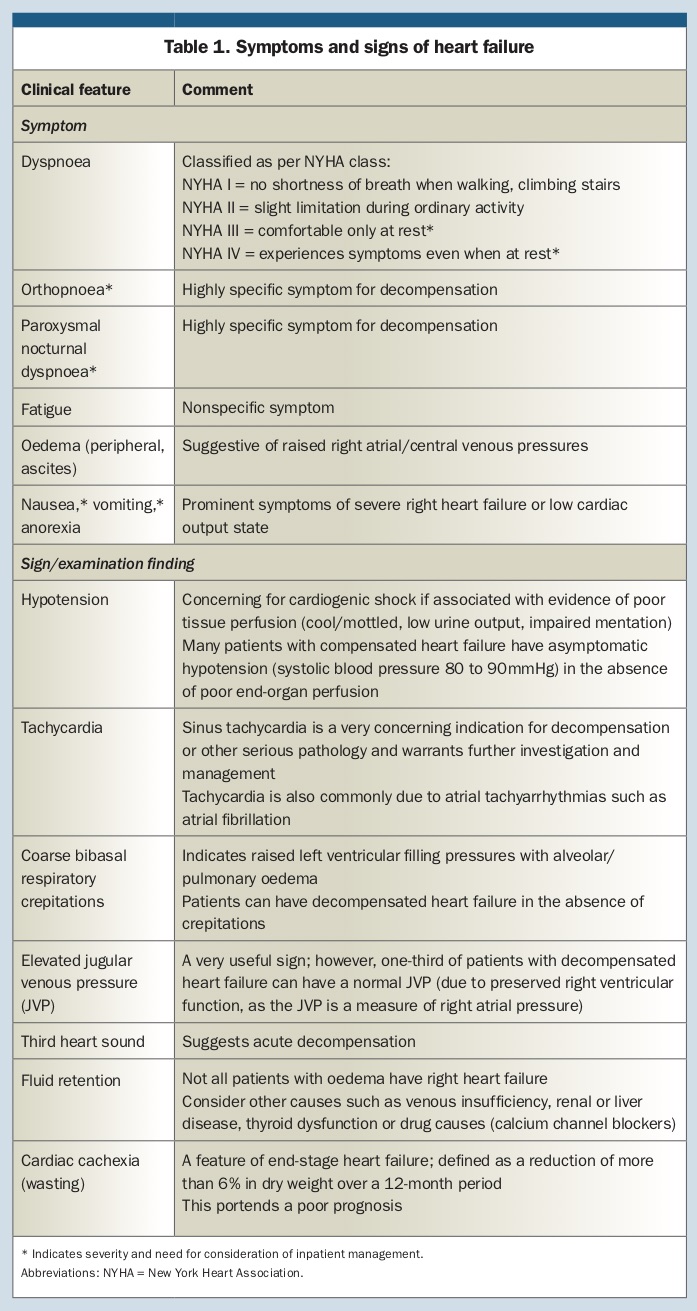
Review of the patient’s fluid balance should be part of the standard review of any patient with heart failure – symptoms and signs of decompensation are listed in Table 1. However, the patient should be empowered to monitor for signs of fluid overload by weighing themself daily. They should notify their treating healthcare practitioner if they gain 2 kg over two days, which should prompt early review.
{kind=link}
Diuretic titration
Diuretics provide symptom relief, leading to reduced hospitalisation (breathlessness accounts for 88% of presentations). Furosemide is generally the first-line agent of choice. A typical starting dose in a ‘diuretic-naïve’ patient is 20 to 40 mg daily orally, with a maximum dose of 500 mg daily in individuals with significant renal dysfunction.
Sequential nephron blockage with an additional agent such as a thiazide diuretic can augment the diuresis. It is important to monitor for renal dysfunction and electrolyte derangement in the setting of diuretic dose titration.
Case scenario continued
Mr JS was admitted to hospital for diuresis. He required a continuous infusion of furosemide and a dobutamine infusion to achieve euvolaemia. During this time period Mr JS’s weight decreased from 74.7 to 68.5 kg, representing almost 10% change in body weight. He had an estimated glomerular filtration rate of 49 mL/min/1.73m2 and a creatinine level of 133 mcmol/L.
Additionally, Mr JS required careful education about heart failure. This was most likely to be successful if it included his next of kin, was tailored to his level of education and presented in terms that he found relatable. Mr JS required extensive input from allied healthcare professionals to ensure he had the appropriate resources to facilitate the purchase of prescription medication to ensure medication compliance.
Identification of precipitants of decompensation and institution of early intervention
The precipitating factors identified to have led to admission with heart failure were shortness of breath (in 88% of patients), fluid overload (32%), infection (19%), ischaemia (10%), rhythm disturbance – for example, atrial fibrillation with a rapid ventricular response rate – (10%) and medication nonadherence (8%).1
Typical precipitants for decompensated heart failure can include:
- acute myocardial ischaemia
- anaemia
- arrhythmias (tachycardia or bradycardia)
- sepsis
- noncompliance with medications (i.e. diuretics or lifestyle recommendations)
- thyroid dysfunction
- drugs and iatrogenic causes (i.e. NSAIDs, corticosteroids, nondihydropyradine calcium channel blockers, introduction of beta blockers when not euvolaemic)
- severe hypertension
- acute kidney injury.
Case scenario continued
During his education sessions, it was identified that Mr JS had a limited baseline understanding of heart failure management. He had not been maintaining a fluid restriction or undertaking daily weigh-ins and he did not understand the warning signals of decompensation. This limited insight and understanding had left him vulnerable to a limited access to medications, resulting in an interruption of diuretic use in the days before his admission.
It was considered whether Mr JS’s systolic cardiac function had deteriorated. Deterioration may have occurred in the context of new ischaemia in the setting of progression of his continued cardiovascular disease or failure of a coronary artery bypass graft, progression of his previously mild aortic stenosis, progression of his pulmonary hypertension from undertreated obstructive sleep apnoea or a new arrhythmia.
Another factor that may have contributed to Mr JS’s admission was significant deterioration in his renal function, contributing to reduced efficacy of diuretics.
Introduction of optimal medical therapy
Medical therapy in patients with heart failure with reduced ejection fraction is largely predicated on the modulation of the neurohormonal system, namely the renin-aldosterone neurohormonal system. These agents have the potential to prevent progression of cardiac remodelling, and in some instances result in reverse remodelling and consequent recovery of systolic function. Accordingly, institution of appropriate medical therapy improves symptoms, reduces morbidity and mortality, and reduces admission to hospital.
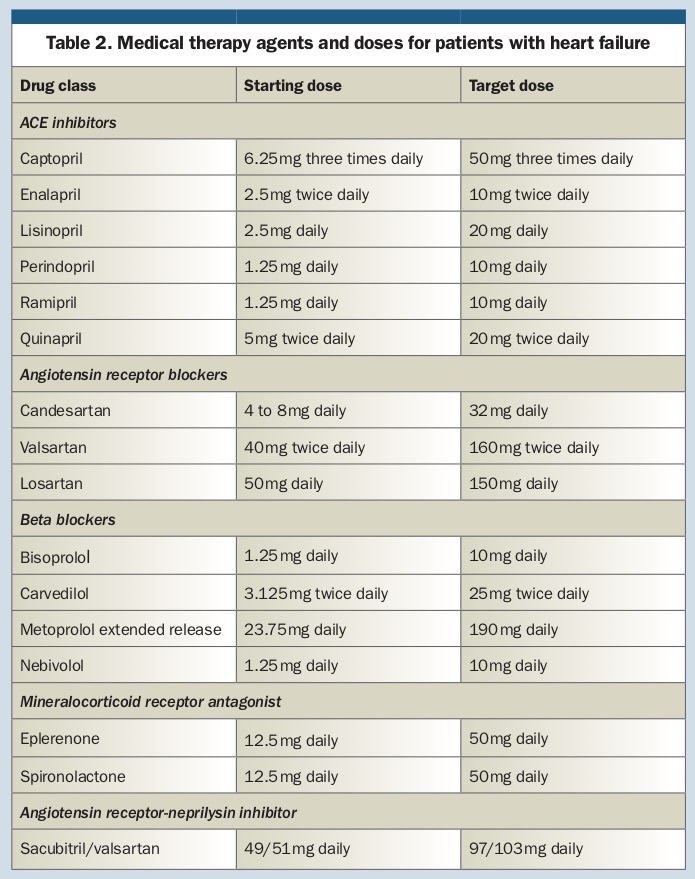
A list of relevant drugs for heart failure and the starting and target doses are given in Table 2.
{kind=link}
ACE inhibitors
An ACE inhibitor should be considered in all patients with systolic heart failure, even if they are asymptomatic. In patients with a left ventricular ejection fraction (LVEF) of less than 40%, ACE inhibitors have been shown to improve symptoms, reduce hospitalisations and reduce mortality rates.2 When initiating therapy with an ACE inhibitor, it is important to monitor a patient’s renal function and for electrolyte derangement.
Beta blockers
Beta blockade, with a heart failure-specific agent, should be considered after starting an ACE inhibitor or angiotensin II receptor blocker in patients with an LVEF of less than 40%. Beta blockers have been demonstrated to reduce mortality and heart failure admissions.2 This therapy should only be initiated once the patient is euvolaemic and at a low initial starting dose, as these agents have the potential to result in decompensation.
Mineralocorticoid receptor antagonist
The use of mineralocorticoid receptor antagonists is well validated in patients with heart failure with reduced ejection fraction, particularly in a cohort of patients with severe (LVEF less than 35%), symptomatic heart failure (New York Heart Association [NYHA] class II to IV). Within the literature, they have been shown to markedly reduce mortality, symptoms and heart failure-related admissions.2
Either spironolactone or epleronone are the agents of choice, with eplerenone having less endocrine side effects such as gynaecomastia. These agents should be used with considerable caution in patients with renal dysfunction (contraindicated in men with creatinine more than 220mcmol/L and women more than 180mcmol/L) and hyperkalaemia (serum potassium levels more than 5.0mmol/L). Accordingly, renal function and electrolytes should be assessed within days of starting this therapy.
Angiotensin receptor-neprilysin inhibitor
Sacubitril/valsartan combination is the first angiotensin receptor-neprilysin inhibitor to recently become available in the Australian market. This new class of drug has changed the landscape for the management of patients with heart failure with reduced ejection fraction, with a landmark trial demonstrating significantly reduced cardiovascular mortality and heart failure-related hospitalisations, when compared with conventional heart failure therapy.3
These drugs should be started in patients with ongoing symptoms (NYHA class II to IV) with documented left ventricular systolic dysfunction, despite maximum tolerated dosage of an ACE inhibitor and a beta blocker. It is important to stop taking the ACE inhibitor at least 36 hours before starting an angiotensin receptor-neprilysin inhibitor, due to the risk of angioedema when used in combination.
Other agents
In those patients who are intolerant of beta blockers, have documented sinus rhythm at a rate of more than 77 beats per minute and have an LVEF of less than 35%, the use of ivabradine can be considered. Digoxin is another agent that can be considered, particularly in those with atrial fibrillation or those who remain symptomatic despite optimal medical therapy. It has a modest inotropic effect and may reduce symptoms.2 It has, however, not been demonstrated to improve rates of mortality.
Case scenario continued
Medication optimisation requires consideration of which standard heart failure medications, with evidence of benefit in the systolic heart failure population, were suitable for this patient (Table 3). ACE inhibitors have proven beneficial and additionally were indicated in the context of Mr JS’s diabetes; however, they were not tolerated due to his significant hypotension and renal dysfunction.
{kind=link}
Beta blockers (bisoprolol 1.25mg daily) were introduced once euvolaemia was achieved and used cautiously in Mr JS given his severe peripheral vascular disease. He was discharged on furosemide 160mg twice daily and spironolactone 25mg daily, as a diuretic with additional mortality benefits.
Treatment with sacubitril/valsartan was not appropriate given Mr JS’s hypotension and renal impairment, but this agent would be considered once a period of stability had been achieved. If Mr JS’s heart rate remained elevated, and his peripheral vascular disease was a limiting factor for further titration of a beta blocker, ivabradine would be considered.
When to refer for cardiology input and hospitalisation
Managing patients with heart failure in the ambulatory setting represents a significant challenge. At times, despite optimal medical therapy and lifestyle measures, hospitalisation is necessary for stabilisation and initiation of additional therapies that are unable to be started in the community.
The following indications should prompt consideration of referral of the patient for admission:
- tachypnoea (respiratory rate >40 breaths per minute)
- hypoxia (oxygen saturation <90%)
- gross fluid overload
- persistent tachycardia
- symptomatic or significant hypotension
- evidence of ischaemia
- end-organ dysfunction (i.e. acute kidney injury, ischaemic or congestive liver dysfunction as manifested by deranged transaminases)
- failure of outpatient therapy.
Concluding comment
Mr JS required multidisciplinary care, not only as inpatient but also in his outpatient management. This case highlights the difficulty of the appropriate co-ordination of care of complex outpatients. Mr JS himself identified that he wanted to have most of his review with his GP, to avoid attending multiple specialist appointments. This raises the importance of clear lines of communication between his specialists and GP, including for support around heart failure medication titration. CT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.