An abnormal ECG and a sudden collapse
Articles in this section are inspired by, but not based on, real cases to illustrate the importance of knowledge about ECGs in relation to clinical situations in general practice. Management is not discussed in detail.
- Isorhythmic dissociation occurs when the sinus node and AV junction are beating completely independently but almost at the same rate, and so the P wave and QRS are moving in and out of phase. It is typically harmless and found in very fit adults.
- Right axis deviation is shown on an ECG by a negative QRS in lead I and a positive QRS in leads II, III and aVF. It is often a normal finding in children and adults with thin, narrower chest walls, as the heart sits more vertically in the chest cavity.
- Other causes of right axis deviation include right ventricular hypertrophy, pulmonary hypertension, acute pulmonary emboli, chronic obstructive airways disease, lateral myocardial infarction, left posterior hemiblock (fascicular block) and congenital heart disease.
- Left posterior hemiblock should be considered as a cause of right axis deviation and it is much more common in older people. It is caused by delayed or nonconduction of the electrical impulse through the inferior and posterior heart muscle. It is a diagnosis that can only be made when right ventricular hypertrophy and other causes of right axis deviation have been excluded.
- An isolated left posterior hemiblock is typically asymptomatic and very rare, as the fibres forming the fascicle that the electrical impulses are conducted through are thicker and relatively resistant to damage compared with the slim single tract that makes up the left anterior fascicle. Left anterior hemiblock is more common.
Jonno is a 23-year-old labourer who has come to the first antenatal visit with his 18-year-old fiancée, Anna, and her mother. Jonno is fit, thin and not very muscular, but appears to be of a healthy weight and is short in stature. He has not been a patient of any medical practice in recent years and does not smoke, take drugs or drink alcohol. He is on no medications and is not aware of any medical issues he might have.
The conversation turns to the standard blood tests requested in early pregnancy. Suddenly everyone hears Jonno snort and his head rolls backwards. He slumps upright in the chair.
Anna and her mother shriek and burst into tears and you drag Jonno off the chair and onto the carpet. Before you can put him into the left lateral position or get oxygen, he has a 30-second, symmetrical, tonic-clonic convulsion and Anna and her mother cry louder (despite your attempts at reassurance).
When the fit is over, Jonno rapidly wakens. He is quite combative and confused, which lasts for about 10 seconds, then his behaviour returns to normal. At this stage, his pulse rate is 40 beats per minute, his oxygen saturation is 96% and his blood pressure is 87/48 mmHg.
Jonno tells you he has never had a fit before and there is no family history of epilepsy. At this point, Anna admits she forgot to mention that Jonno cannot tolerate any talk or sight of blood. Jonno says he had felt a bit faint and thought he could distract himself, but the conversation on the topic went on a bit too long. You ask the nurse to do regular observations on him while you finish the consult with Anna. Jonno is given some milk and biscuits as he has not eaten recently.
When you visit Jonno again, his blood pressure is 95/60 mmHg but his pulse rate is still only 44 beats per minute. He looks well and feels better. His heart sounds are dual, with no murmurs and apex is normal. His chest is clear. Because he is still bradycardic and had collapsed, you decide to do an ECG.
Q1. What conditions could cause Jonno’s collapse and consequent bradycardia?
The most likely cause of this episode is a vasovagal syncope where the bradycardia has been slow to resolve. Jonno is a fit young man who likely has a physiological sinus bradycardia, and so this pulse of 40 beats per minute is an exaggeration of the normal lower baseline, given the vasovagal stimulation related to the blood test discussion.
The short convulsion is not uncommon in this scenario, especially as Jonno was sitting up, with his collapse going unrecognised initially. This would have worsened cerebral hypoperfusion related to the bradycardia and hypotension. His rapid recovery, with no significant postictal phase and his known history of syncope from discussion of blood also all suggest a vasovagal syncope complicated by a short convulsion. This is not epilepsy.
It is less likely that Jonno could have had a tachy-bradyarrhythmia, sinus arrest or some degree of heart block causing bradycardia and consequent collapse. In this age group, hypertrophic cardiomyopathy, long QT syndrome, genetic ion channel mutations (such as Brugada syndrome) and myocarditis should be considered.
Jonno is not taking any medications. However, beta blockers, calcium channel blockers, digoxin, lithium, amiodarone, flecainide, sotalol, mesalamine and acetylcholinesterase inhibitors can all cause bradycardia and potentially syncope.
Q2. What does Jonno’s ECG show?
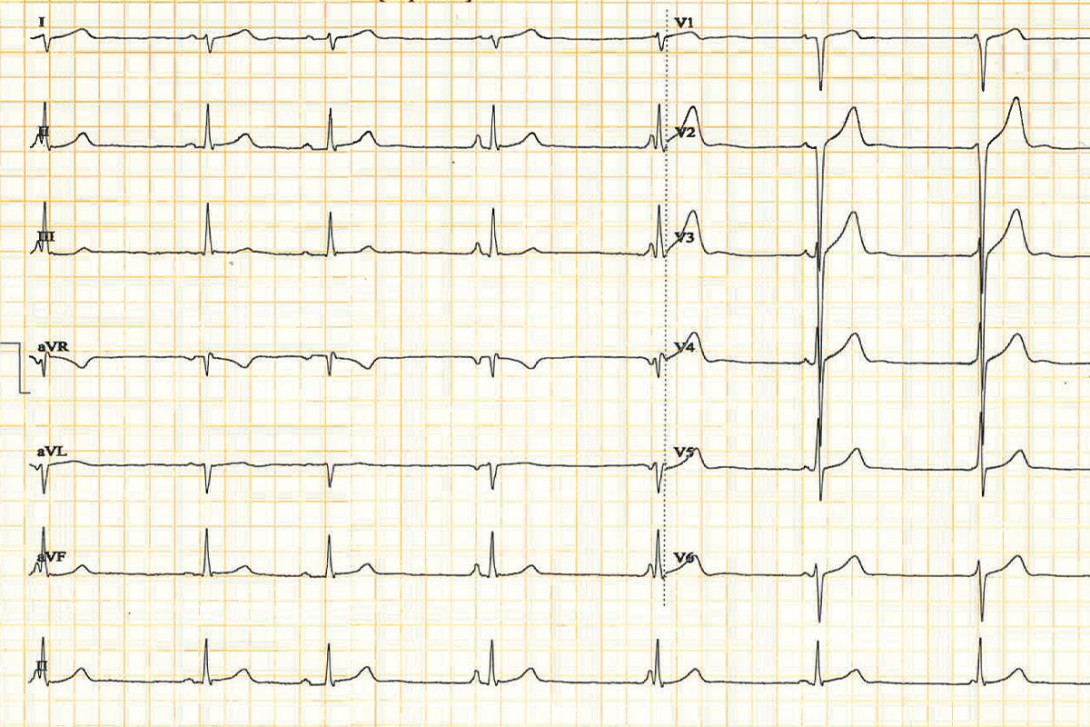
Jonno’s ECG shows the following:
- sinus rhythm with sinus bradycardia (48 beats/minute) and also with isorhythmic dissociation (the sinus node and AV junction are beating independently but almost at the same rate, and so the P wave and QRS are moving in and out of phase)
- atrial ectopic beats (the third and fourth P waves are subtly different from the first and second)
- right axis deviation.
Q3. What is the differential diagnosis of the ECG findings?
Right axis deviation (the QRS in lead I is negative and in leads II, III and aVF is positive) and in this context also the increased right ventricular and septal voltage are often normal findings, as in thin, young people the heart may sit more vertically in the chest. Right axis deviation in isolation in a young person may be described as persisting juvenile changes.
It is possible Jonno has an underlying structural heart disease. Cardiomyopathy can be associated with sudden collapse due to tachy-bradyarrhythmias, hemiblocks and heart block, sinus arrest and reduced left ventricular ejection fraction leading to sudden hypotension (for example, with positional change or with Valsalva manoeuvres such as lifting or straining).
Q4. What, if anything, should be done next?
An urgent resting cardiac echocardiogram was arranged for Jonno. This was normal and excluded right ventricular hypertrophy, congenital heart disease and cardiomyopathy.
Q5. What is isorhythmic dissociation?
Isorhythmic dissociation is a condition where the sinus node and AV junction are beating completely independently but at almost the same rate, and so the P wave and QRS are moving in and out of phase. This can result in the P wave not being visualised periodically as its timing is occurring within the QRS complex. The atrial and ventricular rates are similar, unlike complete heart block. It is normally a harmless condition and found in healthy, very fit young people, especially athletes, and in people during sleep or anaesthesia.
Q6. How would a left posterior hemiblock (fascicular block) be diagnosed if this is benign right axis deviation?
In left posterior hemiblock the electrical impulse is delayed or not conducted through the inferior/posterior heart. There is right axis deviation (the QRS in lead I is negative and in leads II, III and aVF is positive), the rS complex is negative in aVL and there is a small Q wave and tall R wave (qR) in leads II, III and aVF. There is a normal or borderline prolonged (normal is <120 ms) QRS complex duration. Left posterior hemiblock is a diagnosis that can only be made when right ventricular hypertrophy has been excluded and no other cause for the right axis deviation has been found.
Q7. What is the significance of a left posterior hemiblock?
An isolated left posterior hemiblock is very rare, as the fibres forming the fascicle that the electrical impulses are conducted through are thicker and relatively resistant to damage compared with the slim single tract that makes up the left anterior fascicle.1 Hence a left anterior hemiblock is more common. It is often associated with a right bundle branch block and then the prognosis is more serious due to the risk of a complete heart block developing.
An isolated left posterior hemiblock is often due to atherosclerotic heart disease, hypertensive heart disease, aortic stenosis, acute myocarditis, infiltrative conditions (sarcoidosis, amyloidosis) and cardiomyopathy. As previously stated, it is very rare and usually asymptomatic. It may be transient.2 However, research suggests there is an increased risk of sudden cardiac death in young people.3
A true isolated left posterior hemiblock needs further investigation due to possible coronary arterial anatomical abnormalities or genetic conditions. For example, familial progressive cardiac conduction defect (PCCD), also known as Lenègre disease, can be due to mutations in the SCN5A, SCN1B and TRPM4 genes. This condition may progress to complete heart block. Affected individuals may be asymptomatic, or the condition may cause shortness of breath, dizziness, fainting, abdominal pain, heart failure or sudden death.
Outcome
The ECG was repeated after the cardiac echocardiogram and was normal with no ectopic beats, no isorhythmic dissociation and a persisting right axis deviation. An cardiac electrophysiologist was consulted about the case and kindly viewed the ECGs. He felt that no further management or investigation was needed as the patient was highly likely simply to have a persisting juvenile right axis deviation in the presence of the normal cardiac echocardiogram.
Jonno was reassured that the collapse and short convulsion were due to a vasovagal episode related to the conversation about blood. This caused his pulse to slow, his blood pressure to drop and he collapsed. He was urged in future medical consults (and especially in those regarding the pregnancy) to warn the doctor or nurse that he faints with discussions about blood.
If he feels faint in the future in this scenario he should sit down with his head between his legs, or better, lie down on the floor until he feels well again. CT
COMPETING INTERESTS: None.
References
1. Larkin J, Buttner R. Left posterior fascicular block (LPFB). Life in the Fast Lane Dec 9, 2021. Available online at: https://litfl.com/left-posterior-fascicular-block-lpfb-ecg-library/ (accessed February 2026).
2. Pérez-Riera AR, Barbosa-Barros R, Daminello-Raimundo R, de Abreu LC, Tonussi Mendes JE, Nikus K. Left posterior fascicular block, state-of-the-art review: A 2018 update. Indian Pacing Electrophysiol J 2018; 18: 217-230. Available online at: https://pmc.ncbi.nlm.nih.gov/articles/PMC6302819 (accessed February 2026).
3. Calò L, Bona RD, Martino A, et al. Left posterior fascicular block and increased risk of sudden cardiac death in young people. J Am Coll Cardiol 2021; 77: 1143-1145. Available online at: https://www.jacc.org/doi/10.1016/j.jacc.2020.12.033 (accessed February 2026).
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.