Drugs and the heart
Drug reactions
Articles in this section are inspired by, but not based on, real cases to illustrate the importance of knowledge about ECGs in relation to clinical situations in general practice. Management is not discussed in detail.
- Take time with patients who have psychiatric illness or drug problems to obtain a complete medical history early in your care of them.
- It is important to listen to all patients and then investigate appropriately, even if they have difficulty giving you detailed information.
- Do not ignore a short PR interval or prolonged QTc interval on ECGs of patients who have had cardiac events or who have a family history of cardiac events.
- Be aware of medications and illicit drugs that prolong QT intervals; if patients are taking more than one of these regularly, an ECG to check the QT interval is wise.
- Some patients cannot cope with further investigations; remind them gently and positively of the need for these each time you see them.
Jamie is a 50-year-old woman who sees her new GP for a repeat prescription of her opioid replacement therapy. She has a past history of heroin addiction. She has not used any drugs other than marijuana and heroin and has been completely off these now for 10 years. She was successfully weaned onto methadone 20 mg daily at that time.
After two years taking methadone she had a ‘heart attack’, as she understood it, that was presumed to be due to overdose. Jamie had not used amphetamines around the time and cannot recall being unrousable, but says her memory is unreliable from that era. She spent a week in hospital and was placed in drug rehabilitation for another two weeks while her therapy was changed from methadone 20 mg daily to buprenorphine/naloxone 12 mg/3 mg sublingual film once daily. Her records have been lost but she tells her GP that the ‘heart attack’ was presumed to be due to an overdose of methadone. This is corroborated by some old files she has brought.
Jamie takes no medications currently except buprenorphine/naloxone 8 mg/2 mg film once daily and diazepam 5 mg three times daily for anxiety. She is HIV negative and underwent successful eradication of hepatitis C virus two years ago. She has not seen a psychiatrist or addiction specialist for several years as she has been able to reduce her buprenorphine/naloxone dose herself.
The new GP opioid prescriber is concerned about the possible cardiac event eight years ago and assesses her cardiac risk factors. Her lipid levels are: total cholesterol 5.1 mmol/L, HDL-cholesterol 1.3 mmol/L, LDL-cholesterol 2.5 mmol/L and triglycerides 1.4 mmol/L. She has normal results of liver function tests, full blood count, thyroid function tests, iron studies and blood glucose levels. Her blood pressure is normal. She is slim and appears anxious. Cardiorespiratory examination results are normal. Jamie reports her aunt died suddenly of a presumed heart attack at age 55 years, but she is estranged from her family and does not know any other family history. She smokes 10 cigarettes daily and is trying to reduce these with the aid of nicotine gum and patches.
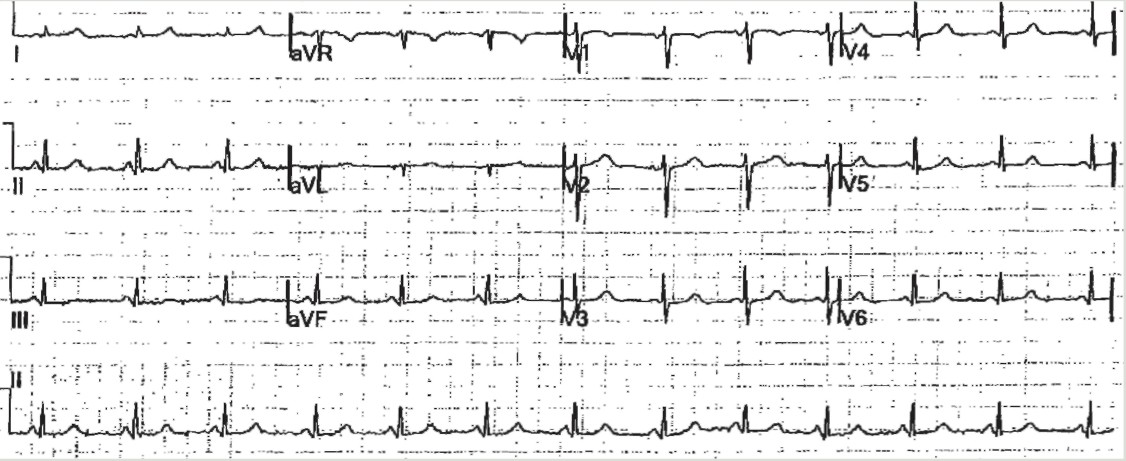
Her new GP performs an ECG as part of the cardiac investigations (Figure).
{kind=link}
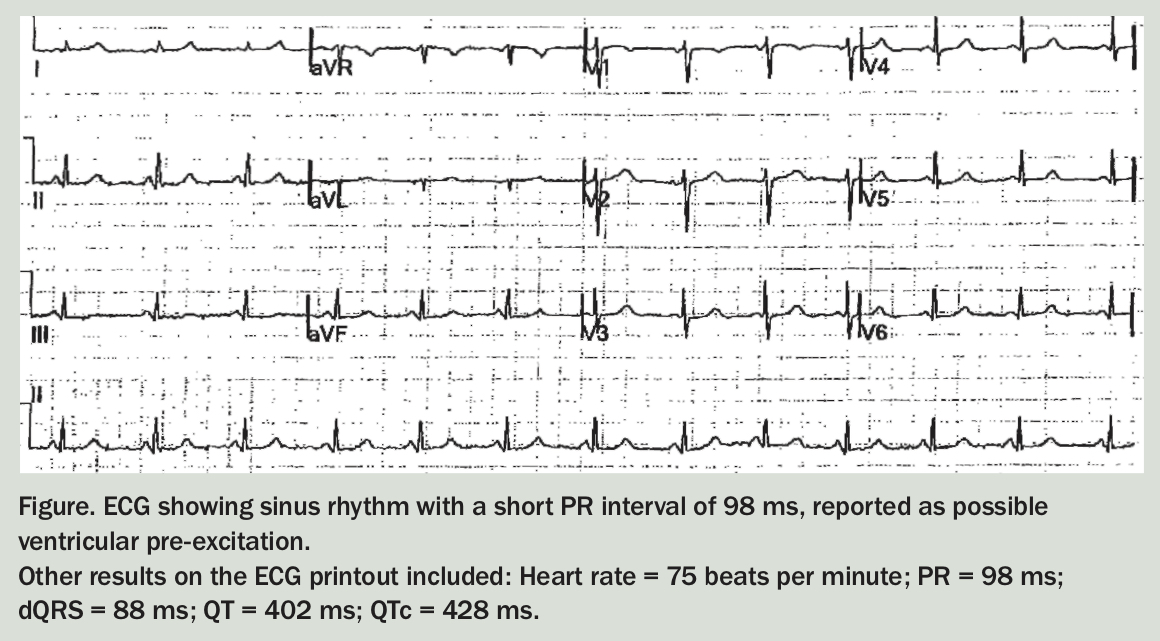
Q1. What does the ECG show?
The ECG shows sinus rhythm, with a heart rate of 75 beats per minute and a short PR interval (98 ms; reference range 120 to 200 ms). Other intervals are normal duration: QRS 88 ms, QT 402 ms and adjusted QT (QTc) 428 ms. The short PR interval suggests the possibility of ventricular pre-excitation.
Q2. What does the PR interval represent?
The PR interval is the time taken from the onset of the P wave to the beginning of the QRS complex. It represents the time taken from the onset of atrial depolarisation to the onset of ventricular depolarisation and reflects conduction through the atrioventricular (AV) node.
The PR interval varies depending on the heart rate and sympathetic nervous system. Faster heart rates due to sympathetic nervous system activation increase conduction through the AV node and shorten the PR interval. Vagal stimulation lengthens the PR interval. The normal PR interval range of 120 to 200 ms takes this variation into account.
Q3. What is the significance of the short PR interval in the light of Jamie’s history?
The significance of a short PR interval depends on the other features of the ECG and the patient’s clinical history:
- In patients with a normal QT interval and QRS complex and no personal or family history of palpitations or other cardiac events, a short PR interval is likely to be a normal variant.
- In patients who have significant coronary artery disease, a short PR interval is associated with increased cardiovascular and all-cause mortality.1
- In patients who have had pathological tachycardias (typically supraventricular tachycardias), a short PR interval suggests a re-entry circuit involving a conduction pathway from atrium to ventricles in addition to the normal atrioventricular nodal path. The most common examples are Wolff-Parkinson-White syndrome and Lown-Ganong-Levine syndrome.
Jamie has not been aware of any significant palpitations, although this does not exclude the possibility that she is prone to them.2 She has an anxiety disorder and hence has heightened sympathetic tone, a possible cause of the short PR interval seen on her ECG. However, her normal heart rate of 75 beats per minute at the time of the ECG makes this explanation unlikely.
Q4. How could medications affect patients who have a long QT interval?
Jamie’s QTc interval of 428 ms is towards the higher end of the normal range (<470 ms in females and <450 ms in males). This could be significant if she requires medications that prolong the QT interval. Many psychiatric medications can prolong the QT interval and if the patient already has a longer than usual QT interval, can precipitate significant arrhythmias. QT prolongation is associated with torsade de pointes. For this reason, many psychiatric medications carry a rare, but definite, risk of cardiac death. There is a long list of medications that can prolong the QT interval and psychiatric patients may easily be taking several of these daily (Box).
Regarding Jamie’s medications, diazepam usually has no influence on the PR or QT intervals. Methadone in high doses can prolong the QT interval.3 It is possible that Jamie’s methadone therapy caused an arrhythmia responsible for her ‘heart attack’. This is even more likely if her consciousness was impaired, which is a possible reason why a methadone overdose was suspected at the time of the event. Interestingly, her addiction specialist appears to have considered this possibility and changed her from methadone to buprenorphine/naloxone therapy. Buprenorphine has less risk of QTc prolongation compared with other opioids.4
Q5. How should Jamie best be managed at this point?
Jamie has already undergone basic blood tests for cardiovascular risk, with normal results. A cardiovascular examination also has normal results. Jamie should now undergo 24-hour Holter monitoring (to identify possible asymptomatic pathological arrhythmias) and resting cardiac echocardiography, arranged before prompt referral to a cardiologist. Given her history of ‘heart attack’, her current age and family history of early cardiac mortality, further investigations such as a coronary artery CT scan or a stress ECG may be indicated to assess whether she has any significant coronary artery disease. A referral to a cardiologist specialising in electrophysiological studies should also be considered, particularly if Holter monitoring shows arrhythmias.2
Outcome
The GP refers Jamie for a cardiac echocardiogram, which does not show any abnormalities. Jamie does not want to have 24-hour Holter monitoring. She struggles with change and uncertainty and is too anxious about further investigations to even see a cardiologist. Her GP continues to offer to make her an appointment with a cardiologist each time she attends for repeat prescriptions. CT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.