Arboviral infections and the heart
Dr Miller is a GP in Sydney, a medical journalist and author, and the Medical Editor of Cardiology Today.
Traveller’s health
Articles in this section are inspired by, but not based on, real cases to illustrate the importance of knowledge about ECGs in relation to clinical situations in general practice. Management is not discussed in detail.
- Consider the potential for arboviral infection causing heart complications in unwell travellers, especially pregnant women and people with pre-existing heart disease.
- Serology is the main diagnostic method, but Zika virus serology may cross-react with dengue fever or even yellow fever immunity, appearing to be positive for those diseases instead.
- Arboviral infection affecting the heart may cause arrhythmias, heart block or cardiac failure (either from complicating existing myocardial disease or due to myocarditis or pericarditis).
- Cardiac complications of arboviral infections typically resolve when the acute infection has resolved.
John is a 68-year-old nonsmoker with stable ischaemic heart disease. Five years ago, he was infected with adenovirus and he has had stable cardiomyopathy since then. He takes apixaban 5 mg twice daily and sotalol 80 mg twice daily for prevention of atrial fibrillation. He also takes atorvastatin 40 mg daily and omega 3 and 6 fish oil supplements.
John and his wife recently spent four weeks travelling across Malaysia by car and ferry before flying home. He was bitten by mosquitoes throughout the trip. Five days before his return, he became sick with a low-grade temperature, myalgia, nausea and headache. On arrival back in Australia, he immediately presents to his GP complaining of shortness of breath and constant central chest heaviness with no radiation for the past two days.
{kind=link}
Outcome
John’s cardiac enzyme levels were mildly elevated, his full blood count showed a mild increase in his total white cell count with a mild lymphocytopenia and mild thrombocytopenia and he had a C-reactive protein level of 65 mg/L (normal range, <6.0 mg/L). Results of other investigations were normal.
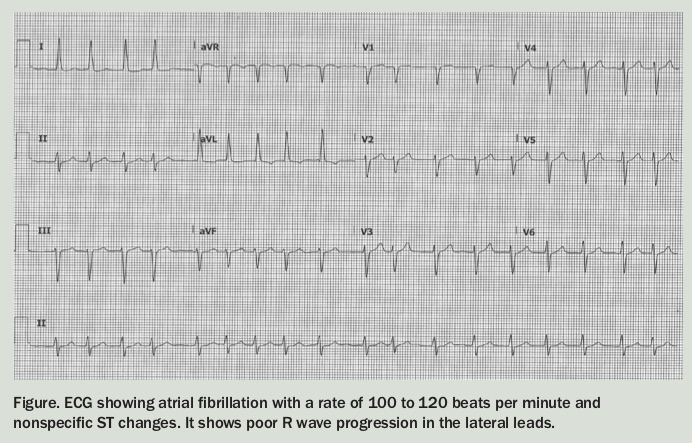
His paired Zika virus serology later came back positive. The cardiac echocardiogram showed a reduced ejection fraction of 50% (his usual being 60%) and his AF at this time had reduced to about 90 beats per minute. He was maintained on sotalol 160 mg twice daily.
John was monitored in hospital and discharged several days later after the AF had spontaneously reverted to sinus rhythm. At this time his cardiac echocardiogram showed an ejection fraction of 60% again and his cardiac enzymes were normal. He was advised to strictly avoid mosquito bites in any future travels to Zika-affected regions. CT
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.