Percutaneous mitral valve interventions
Heart valve diseases
Heart diseases
In patients who are high risk for open cardiac surgery, percutaneous mitral valve repair is now available as an effective treatment for severe mitral regurgitation. These minimally invasive procedures are performed by specialist teams in tertiary cardiac hospitals and improve quality of life and prognosis in appropriately selected patients.
- Mitral regurgitation (MR) is a common form of valvular disease that affects blood flow to the body.
- MR can be acute (requiring inpatient care) or chronic (can be managed in the outpatient setting) and ranges from mild to severe. Although patients with mild MR can be managed through active surveillance, those with severe MR may need further intervention.
- Transcutaneous mitral valve repair improves symptoms and the prognosis in selected patients with severe MR.
- The procedure is performed via keyhole access through the femoral vein and is technically successful in around 95% of patients with a major complication rate of around 3%.
- Patients are typically discharged from hospital 24 to 48 hours after the procedure and may return to unrestricted activities after two weeks.
- Patients require yearly surveillance echocardiography with mitral valve assessment after the procedure.
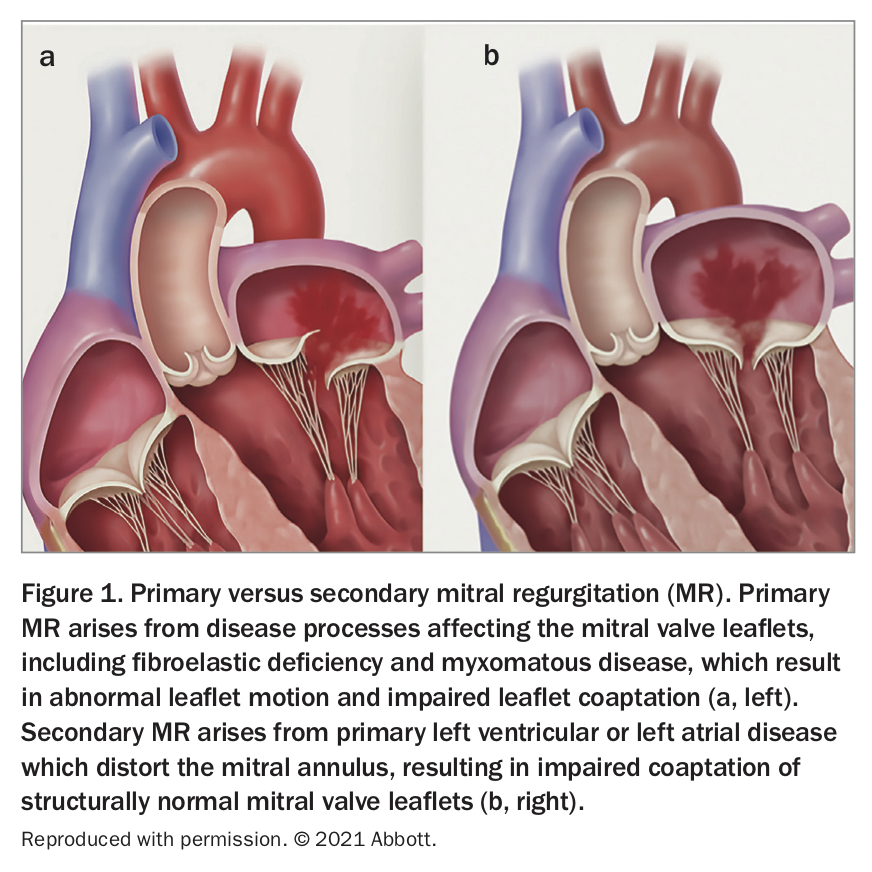
Mitral regurgitation (MR) is a common form of valvular heart disease, characterised by abnormal passage of blood from the left ventricle to the left atrium during ventricular systole. MR may be acute or chronic and may arise from disease processes that affect the mitral valve leaflets (primary MR) or from left ventricular or left atrial disease which distort the mitral annulus or subvalvular apparatus (secondary MR) (Figure 1). Acute MR is a cardiac emergency requiring inpatient care and surgical evaluation, whereas chronic MR is primarily managed in the outpatient setting by cardiologists and general practitioners.
{kind=link}
Mitral regurgitation severity is evaluated with clinical assessment and echocardiography. Mild to moderate MR is often well tolerated and may be managed with active surveillance. Severe MR is a serious, progressive condition that causes left ventricular failure, pulmonary hypertension, atrial arrhythmia and premature cardiac mortality. Presenting symptoms of this disease include dyspnoea, impaired functional capacity and peripheral oedema. Mitral valve surgery with either valve replacement or repair is the gold standard for treatment of severe mitral regurgitation and alleviates morbidity and mortality in selected patients.1 In many cases, however, patients are precluded from surgical intervention due to unacceptable perioperative risk.2 Furthermore, the benefit of surgical intervention in patients with heart failure who have secondary MR is unclear.1,3,4 In these patient groups, percutaneous mitral valve intervention is now available as an effective treatment for severe MR.5 These interventions include the well-established percutaneous edge-to-edge repair and the evolving technologies of transcatheter mitral valve annuloplasty and valve replacement.
Mitral regurgitation assessment
After history taking and clinical examination, patients should undergo comprehensive transthoracic echocardiography to formally evaluate the severity and mechanism of MR. Transthoracic echocardiography is the first-line test for evaluation of all valvular disease, and may characterise MR severity as mild, moderate or severe, based on a combination of qualitative (colour Doppler) and quantitative (regurgitant volume, effective regurgitant orifice area) parameters.6 If significant MR is identified, further assessment with transoesophageal echocardiography should be considered. Transoesophageal echocardiography is an endoscopic procedure performed under procedural sedation with an ultrasound probe inserted into the patient’s oesophagus and stomach. It facilitates exquisite, high-definition mitral valve imaging, allowing detailed mitral valve anatomical assessment and precise definition of the mechanism of MR. Additionally, 3D mitral valve imaging by transoesophageal echocardiography is crucial in evaluating technical feasibility of mitral valve surgery or transcutaneous mitral valve repair.7
Percutaneous edge-to-edge mitral valve repair
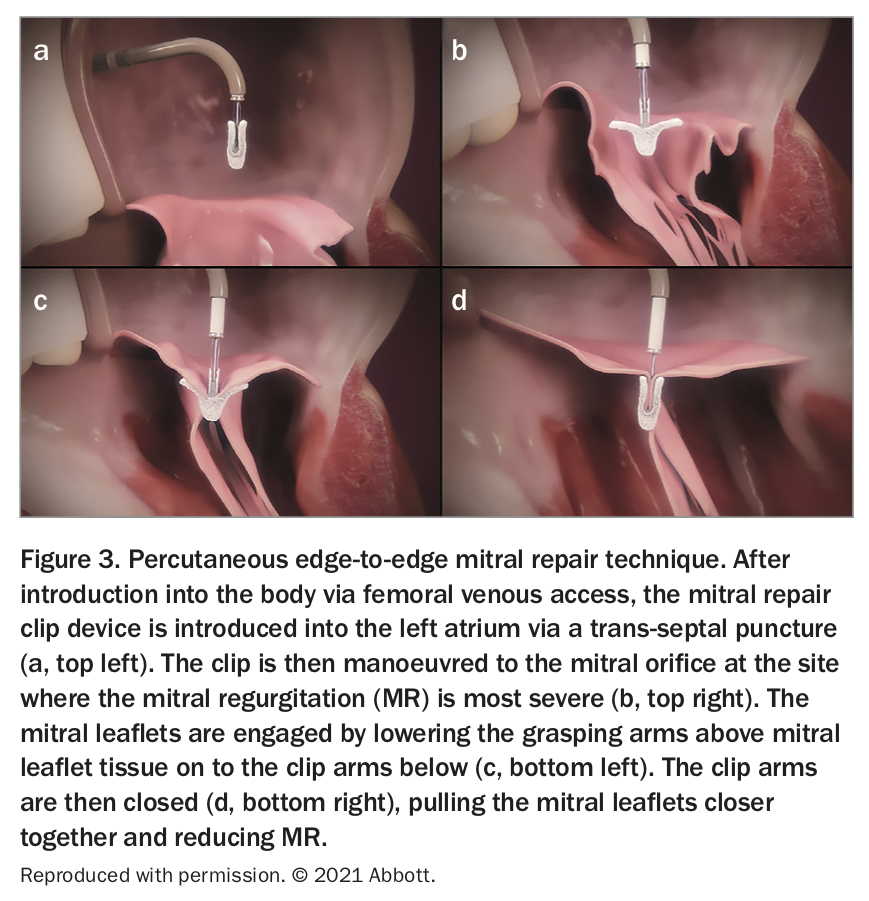
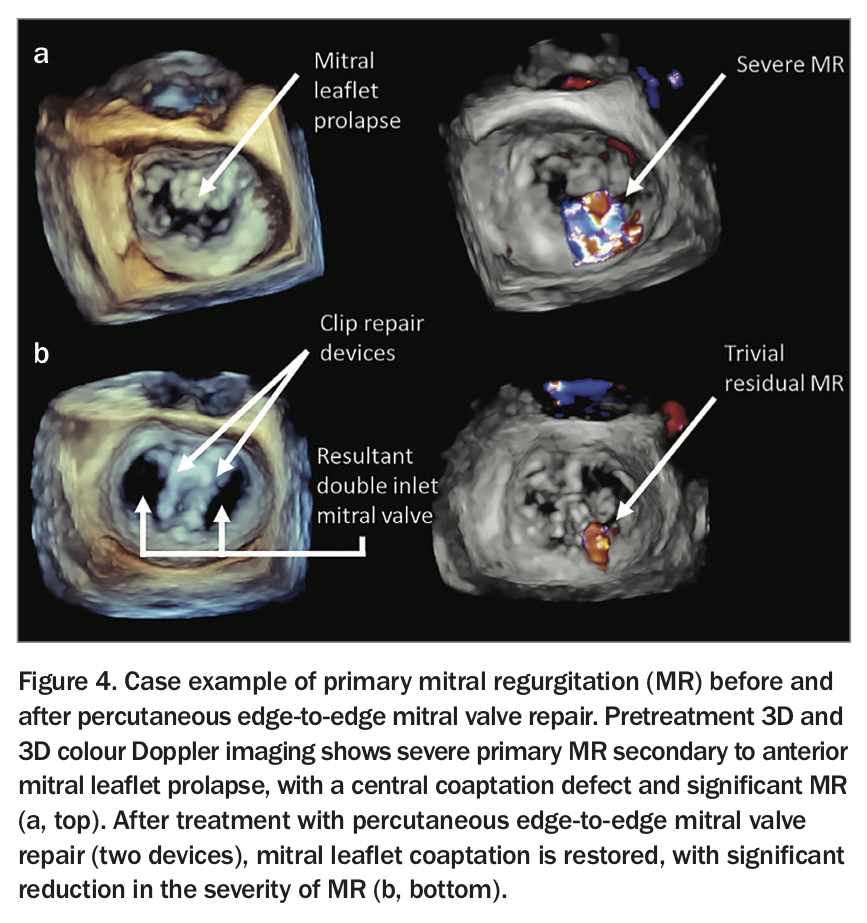
Percutaneous edge-to-edge mitral valve repair may be undertaken in a tertiary-level cardiac hospital with cardiothoracic surgical capability. The procedure is performed under general anaesthesia by a team of interventional cardiologists, imaging cardiologists, anaesthetists and nurses in a hybrid cardiac catheterisation operating theatre. To perform the procedure, a clip device with two symmetrical arms designed to grip and oppose the mitral leaflets (Figure 2) is introduced via a delivery system into the femoral vein, passed through the inferior vena cava into the right atrium, and then across the inter-atrial septum via a trans-septal puncture to reach the left atrium. Once in the left atrium, the clip is manoeuvred under real time 3D transoesophageal imaging guidance to the mitral valve orifice and orientated toward the site where the MR is most severe. The clip is deployed by engaging tissue from both mitral leaflets and pulling the leaflets closer together, thereby improving leaflet coaptation and reducing the severity of MR (Figure 3). 3D transoesophageal imaging of percutaneous edge-to-edge mitral valve repair in a patient with primary MR is shown in Figure 4.
{kind=link}
{kind=link}
{kind=link}
Patient selection and procedural efficacy
Currently, patients with severe MR who are considered high risk for surgery may be considered for percutaneous mitral valve repair. In patients with primary MR, mitral valve anatomy is the key determinant in patient suitability for these angiographic procedures. Features including mitral leaflet length, mitral leaflet calcification and the presence of concomitant mitral stenosis are important anatomical considerations.7 In secondary MR, left ventricular evaluation is also an important component of patient selection. Secondary MR is primarily a disease of the left ventricle. Given this, surgical treatment of secondary MR has historically been ineffective in altering disease course, with primary left ventricular disease governing prognosis.4 Percutaneous mitral valve repair, however, alleviates the haemodynamic consequences of MR without associated surgical morbidity, and has been shown to improve symptoms and prognosis in selected patients with secondary MR.8 Patients with secondary MR who benefit most from percutaneous edge-to-edge repair are those in whom primary mitral valve dysfunction, in addition to left ventricular disease, is found to be contributing to the severity of valvular regurgitation.8-10
Patient suitability for percutaneous mitral valve intervention should be determined by consensus discussion among a ‘heart team’ involving interventional and imaging cardiologists, cardiothoracic surgeons, allied health professionals and, where appropriate, geriatricians.5 Appropriately selected patients for percutaneous mitral valve repair receive significant benefit from the procedure, with improved functional class, quality of life, and prognosis compared with patients receiving medical therapy alone.8 Evidence shows that preprocedural optimisation of heart failure medical therapy with beta blockers, ACE inhibitors and mineralocorticoid receptor antagonist as indicated improves patient outcomes after percutaneous mitral valve repair; therefore, optimisation of medical therapy should be undertaken before consideration of this procedure.8
Percutaneous mitral valve repair rarely completely abolishes MR, and a reduction in MR severity from severe to mild or mild-moderate grade is considered a technically successful procedure. Technical success is obtained in around 95% of patients who undergo the procedure, with implantation of one or two clips typically required.8,9 Immediate risks of the procedure include vascular access complications, pericardial effusion or tamponade, iatrogenic mitral stenosis, emergency cardiac surgery and death, with a major complication rate of around 3%.8,9
Follow up and monitoring
Patients who undergo percutaneous mitral valve repair typically need 24 to 48 hours of monitoring in hospital before discharge and should limit heavy lifting for two weeks after the procedure. Echocardiography should be performed in hospital on the day after the procedure to assess procedural success and screen for complications such as pericardial effusion. Late-stage complications of percutaneous mitral valve repair are uncommon; however, dislodgement of a clip arm and recurrent severe MR is rarely encountered, and surveillance echocardiography should therefore be performed on an annual basis. Patients may require aspirin therapy for six months after percutaneous mitral valve repair.11,12 Patients may experience a reduction in diuretic requirement after the procedure owing to improvement of their cardiac function. Any heart failure-modifying medications taken before the procedure, however, should typically continue at preprocedural doses. Long-term follow up studies of outcomes are currently limited given the recent development of this procedure; however, clinical experience demonstrates many patients receive sustained symptomatic and prognostic benefit for many years after percutaneous mitral valve repair.13
Emerging percutaneous mitral valve intervention
In addition to edge-to-edge repair, numerous other techniques for percutaneous mitral valve intervention are being explored. These techniques include percutaneous mitral annuloplasty, percutaneous mitral chordae replacement, and full percutaneous mitral valve replacement.14 These techniques are currently predominantly limited to clinical trial settings; however, they may represent future treatment alternatives for patient with severe MR in cases where surgical intervention or percutaneous edge-to-edge repair is not feasible.
Conclusion
The need for intervention in patients with MR is dictated by the severity of disease: patients with mild MR can be managed with active surveillance; however, those with severe MR may require intervention. In patients with severe MR who are at high risk for operative intervention, percutaneous mitral valve repair can improve symptoms, prognosis and quality of life. These procedures are performed by teams of cardiac specialists in tertiary cardiac referral centres. Postprocedural follow up includes immediate (next-day) echocardiography to identify complications and annual surveillance echocardiography to evaluate durability of repair. CT