Cardiovascular disease and COVID-19: summary of the Australian and New Zealand consensus statement

COVID-19
A consensus statement, developed by Australian and New Zealand expert bodies, was published in August 2020 to review the evidence on SARS-CoV-2 infection and cardiovascular disease and make recommendations on cardiac service provision during the COVID-19 pandemic. This summary of the statement focuses on issues relevant to GPs.
- Pre-existing cardiovascular disease is a significant risk factor for the development of severe illness and death following infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
- ACE inhibitor and angiotensin-receptor blocker therapy should be continued in patients with COVID-19.
- COVID-19 can manifest with or be complicated by several cardiac conditions, particularly acute myocardial injury.
- The degree of cardiac troponin elevation is a marker of prognosis in patients with COVID-19; however, routine measurements should not influence treatment decisions.
- Therapies being used for the treatment of COVID-19 can have significant cardiac adverse effects.
- The COVID-19 pandemic has affected the provision of cardiovascular health care and care-seeking by patients; primary care doctors are in an important position to protect the cardiovascular health of the community during the pandemic.
The coronavirus disease 2019 (COVID-19) pandemic has significant implications for cardiovascular care in the community, through both direct and indirect effects. Patients with pre-existing cardiovascular disease (CVD) are known to have significantly higher rates of adverse outcomes after infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1 SARS-CoV-2 infection can lead to a range of acute cardiovascular complications with long-term prognosis as yet unknown.2 Medications used to treat COVID-19 can have adverse cardiovascular effects. Moreover, the societal impacts of the pandemic have indirect effects on cardiovascular health. Patients with either acute or chronic cardiovascular illness may avoid seeking medical attention or attending follow-up because of government-mandated restrictions or anxiety about the risk of nosocomial infection.3 There are also implications for the provision of timely cardiovascular care, as increased precautions and measures to preserve hospital supplies of personal protective equipment may affect service delivery.
The Australian and New Zealand consensus statement on cardiovascular disease and COVID-19, published in August 2020, reviewed the evidence on SARS-CoV-2 infection in patients with pre-existing CVD and the acute cardiovascular effects of COVID-19, and made recommendations for cardiac service provision during the pandemic.1 It was endorsed by the Cardiac Society of Australia and New Zealand, Australian and New Zealand Society of Cardiac and Thoracic Surgeons, National Heart Foundation of Australia and High Blood Pressure Research Council of Australia. Here, we summarise the consensus statement, with an emphasis on issues relevant in primary care.
Pre-existing cardiovascular disease and COVID-19
Patients with pre-existing CVD have a significantly increased likelihood of developing severe illness or dying from COVID-19. In a meta-analysis of eight studies involving more than 46,000 patients in China, the odds ratio (OR) for developing severe versus mild illness was higher for those with pre-existing CVD (OR, 3.42; 95% confidence interval [CI], 1.88 to 6.22) than for those with any other comorbidity, including hypertension (OR, 2.36; 95% CI, 1.46 to 3.83) and respiratory disease (OR, 2.46; 95% CI, 1.76 to 3.44).4 The case fatality rate among patients with CVD was 4.4 times higher than that of the overall cohort.5 Similarly, in a study of hospitalised COVID-19 patients in New York, pre-existing CVD was the second strongest predictor of in-hospital mortality after chronic pulmonary disease.6 A degree of confounding by older age and male sex, both risk factors for CVD and severe COVID-19, may partly explain these findings.7 Nevertheless, pre-existing CVD still conferred a significant risk of more severe COVID-19 after adjustment in a pooled analysis of four studies (relative risk [RR], 1.75; 95% CI, 1.12 to 2.73).7
The mechanisms responsible for the increased risk in patients with pre-existing CVD have not been fully elucidated. However, the high incidence of myocardial injury described in severe COVID-19 likely plays a part in patients who already have compromised cardiovascular reserve.
Although further studies are needed to determine the precise relationship between pre-existing CVD and poor COVID-19 outcomes, it is important to include patients with pre-existing CVD in the ‘vulnerable’ population who require a particular emphasis on preventing SARS-CoV-2 infection and a low threshold for testing.
ACE inhibitors and angiotensin receptor blockers
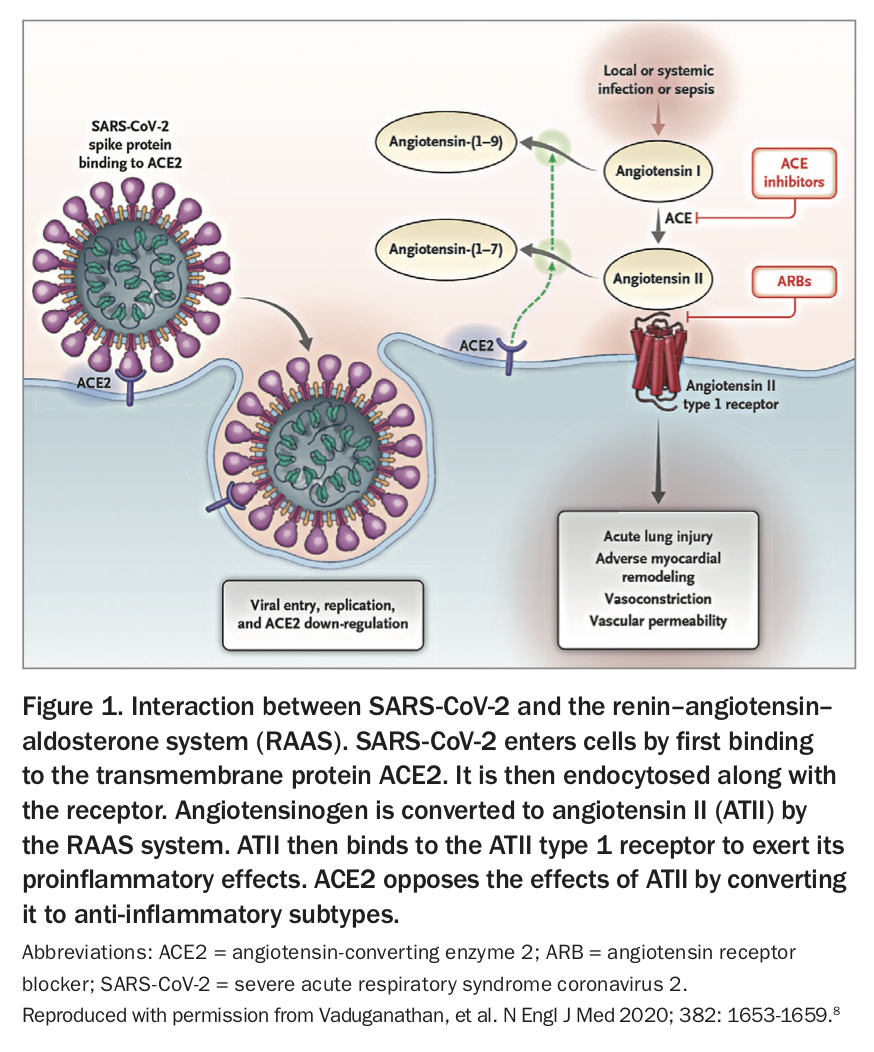
Angiotensin-converting enzyme 2 (ACE2) is an integral membrane protein that inactivates angiotensin II, abating its vasoconstrictive effects. The SARS-CoV-2 virus responsible for COVID-19 enters human hosts by binding to ACE2 receptors highly expressed in lung alveolar cells (Figure 1).8
{kind=link}
In the initial stages of the pandemic, it was hypothesised that ACE inhibitors and angiotensin receptor blockers (ARBs) might upregulate ACE2 expression, facilitating viral entry.9 However, both animal and human studies of long-term use of ACE inhibitor and ARB medications have shown inconsistent effects on plasma ACE2 levels.10 Several large observational studies have also shown no association between ACE inhibitor or ARB use and COVID-19 severity or mortality.11-13
Thus, the Cardiac Society of Australia and New Zealand (CSANZ) along with a number of international societies have recommended continuation of ACE inhibitor and ARB therapy, as these medications have well-established benefits.1
Cardiovascular implications of COVID-19
COVID-19 can manifest with, or be complicated by, several acute cardiac syndromes including:
- acute myocardial injury (acute nonischaemic myocardial injury and acute myocardial infarction)
- arrhythmias
- pericardial effusion or tamponade
- thromboembolic complications
- heart failure
- cardiogenic shock.14
Myocardial injury in COVID-19
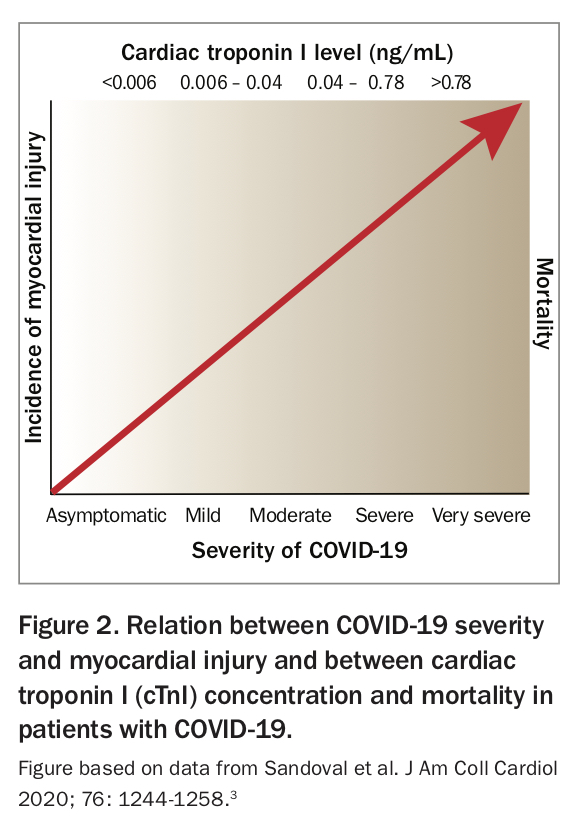
Acute myocardial injury is defined as the presence of cardiac troponin (cTn) concentrations greater than the 99th percentile upper-reference limit that are dynamic.15 Acute myocardial injury is common in people with acute respiratory disease, particularly in critically ill older patients and those with comorbidities.3 Acute myocardial injury has been reported in 10 to 28% of hospitalised patients with COVID-19 and is more common in those with pre-existing CVD and more severe COVID-19 (Figure 2).3,16-18 Importantly, the presence or absence of acute myocardial injury in COVID-19 appears to have a drastic effect on mortality as well as complications, such as the requirement for ventilation and acute kidney injury (Figure 3).3,18
{kind=link}
{kind=link}
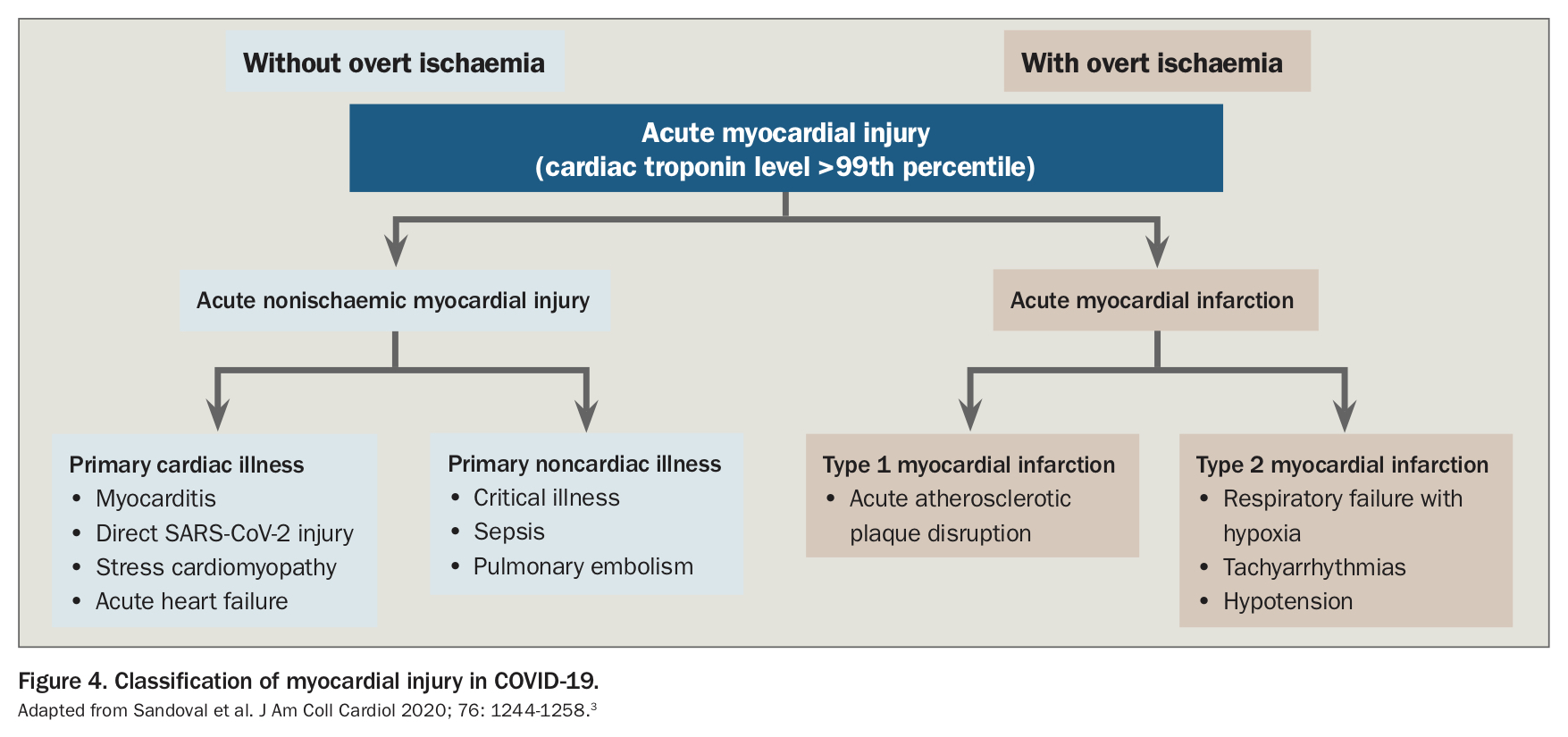
With respect to aetiology, acute myocardial injury in COVID-19 can be classified as:
- acute nonischaemic myocardial injury, which can result from
– cardiac causes (e.g. myocarditis, stress cardiomyopathy and acute heart failure)
– noncardiac causes (e.g. critical illness, sepsis and pulmonary embolism) - acute myocardial infarction (MI), which includes
– type 1 (acute atherothrombosis) MI
– type 2 (myocardial oxygen supply-demand mismatch) MI (Figure 4).3
{kind=link}
Although there is biological plausibility for an increased risk of type 1 MI in COVID-19, this has not yet been reported.3 Conversely, there has been a worldwide reported decrease in the incidence of type 1 MI during the pandemic, thought to be due to symptomatic patients not seeking medical attention because of social-distancing restrictions or fear of nosocomial infection.19-22
Factors that can contribute to the risk of type 2 MI in patients with COVID-19 include hypoxia, acidosis, hypo- or hypertension and the release of inflammatory mediators (e.g. catecholamines, tumour necrosis factor and interleukins). Other causes such as embolic coronary thrombosis and microvascular dysfunction have been reported but are thought to be uncommon.3
It is important to remember that many of the causes of acute cardiac injury in COVID-19 can mimic an acute ST-elevation myocardial infarction (STEMI). An Italian Study found that in SARS-CoV-2-positive patients who presented with acute STEMI, up to 40% had no identifiable culprit lesion on coronary angiography.23 Therefore, patients with acute MI combined with flu-like or fever symptoms should have COVID-19 considered in the differential diagnosis.
Cardiac troponin measurement in COVID-19
The serum troponin level is commonly elevated in patients with COVID-19, with a continuous relationship between cTn concentration and outcomes (Figure 2).18 Studies have shown that the degree of cTn elevation is a marker of prognosis in patients with COVID-19.3,24 However, routine troponin measurements do not change treatment decisions and may expose patients to the risks associated with downstream testing, such as invasive coronary angiography. Therefore, although cTn measurement is not discouraged, it should be used more as a prognostic marker in patients with COVID-19.
Cardiovascular implications of novel COVID-19 therapies
Novel therapies for the treatment of COVID-19 can have cardiac sequelae. Medications such as chloroquine, azithromycin and antiviral medications (e.g. lopinavir, ritonavir and remdesivir) can cause cardiac toxicity, particularly QTc prolongation and torsades de pointes, especially in patients with renal or hepatic dysfunction.1 This in turn can lead to life-threatening ventricular tachycardia, ventricular fibrillation and sudden cardiac death. Clinical trials are underway assessing the utility of these agents in preventing or treating COVID-19.25
It is important that primary care physicians are aware of the potential cardiovascular side effects of these medications, as patients in the community may be enrolled in prophylaxis trials, and hospitalised patients may complete their course of trial medication after discharge.
Implications for cardiovascular healthcare services
In response to the COVID-19 pandemic, cardiovascular healthcare systems around Australia have been rapidly adapted. The primary goal is to maintain the safety of staff and patients by limiting their exposure to COVID-19 and to conserve personal protective equipment and hospital bed capacity. Elective cardiac procedures and surgery may be cancelled or postponed at different stages of the pandemic. As a consequence, much more responsibility falls on primary care doctors to follow up these patients and monitor for acute deterioration of symptoms that warrant more urgent treatment.
A crucial concern is that patients with acute MI are taking longer to present to hospital, with some countries reporting an increase in time from symptom onset to first medical contact, and the rate of out-of-hospital cardiac arrest.22,26,27 Primary care doctors are in an important position to reiterate to their cardiac patients that it is both safe and crucially important that they present to hospital in the event of acute cardiac symptoms or deterioration.
Primary care doctors commonly refer patients for cardiovascular stress testing, ambulatory ECG monitoring and echocardiography. These are likely to be dynamically limited in line with the degree of community transmission of SARS-CoV-2. Exercise stress testing poses a particularly significant risk of viral transmission because of droplet spread. Pharmacological stress testing (pharmacological nuclear stress myocardial perfusion scanning or dobutamine stress echocardiography) avoids the need for exercise or a technician in close proximity and may be relatively safer.1
Another important consideration is the use of telehealth. Once again, dependent on the level of community SARS-CoV-2 infection, telehealth is likely to play a major role in initial assessment and follow up of patients with CVD, in both primary and specialist cardiology care. Although telehealth is an effective way of reducing the risk of infection among vulnerable patients with CVD and health workers, it presents challenges. The efficacy of telehealth consultations for patients with CVD can be improved by using tools to monitor patients such as home blood pressure monitors, weight diaries, more frequent pathology tests and digital health tools that engage patients in their secondary prevention strategies and track compliance.28 Telehealth also allows for more frequent follow up and titration of medications. Both the educational and physical components of cardiac rehabilitation can be delivered via video conferencing. It is also important that patients are supported in accessing home exercise equipment during the pandemic.
Conclusion
Patients with pre-existing CVD are among the most susceptible to severe illness and death as a result of COVID-19. Their risk of infection must be minimised while concurrently ensuring that the care of their cardiovascular condition is not compromised, as this can also lead to increased morbidity and mortality. COVID-19 itself can result in a significant and diverse range of cardiovascular complications with unknown long-term sequelae. The provision of cardiovascular health care has been affected by the pandemic; however, we need to continue to provide high-quality cardiovascular care to the community. CT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.