Sudden severe chest pain: an important symptom to always take seriously

Vascular diseases
Articles in this section use cases to illustrate the emergency management of patients presenting in general practice with cardiac problems. They are inspired by, but not based on, real patient situations.
The case
The ambulance rings ahead to the hospital, where you are a GP working your regular shift in the emergency department. They are bringing in a 53-year-old man with severe chest pain from a local general practice. His GP has sent a letter with the ambulance crew.
The man is known to the practice, but he only presents every year or two with minor complaints. He is a landscape gardener who was working ‘just down the road’ when his symptoms started. He mentioned to his workmate that he didn’t feel quite right, and his colleague took him to see his GP.
The letter reports that the patient presented complaining of central chest pain. He has a background of essential chronic hypertension, which is treated with candesartan 32 mg daily. He has no other medical conditions and no history of hospitalisations. He is an active smoker (20 cigarettes per day, 30+ pack-year history) and he drinks three standard drinks per day. The patient is currently living alone and is feeling stressed because he is going through a divorce and experiencing financial pressures. He has no family history of cardiovascular disease, and both of his parents and all of his siblings are alive and well.
On review with his GP, the patient’s vital signs were blood pressure 130/60 mmHg, heart rate 94 bpm and respiratory rate 22 breaths per minute. The GP performed an ECG, which showed sinus rhythm at 92 bpm with no abnormalities detected, and in particular, no ST segment changes or other signs of ischaemia. The GP administered sublingual glyceryl trinitrate 300 mg and aspirin 300 mg while waiting for the ambulance to arrive. There was no change in the patient’s symptoms.
The paramedics quickly inserted a cannula and administered morphine 10 mg intravenously, in 2.5 mg aliquots, titrated to effect. The patient’s vital signs remained unchanged, with an oxygen saturation of 98%. An ECG repeated in the ambulance showed no change from the first ECG.
What happens in the emergency department?
On arrival at the emergency department, the patient is in distress. He is sweaty and complaining of severe chest pain radiating up into his neck. He is assessed as triage category 1 and wheeled straight into the resuscitation area. The paramedic team give handover to the resuscitation team after transferring the patient onto the hospital bed. An initial set of vital signs show there has been no change from the time he presented at the practice and indicate that he is haemodynamically stable.
You ask the patient about the details of his presentation. He says that he has severe ‘11 out of 10’ pain in the middle of his chest. The pain came on suddenly, but he is unable to characterise the type of pain. He says the pain initially radiated to the left side of his neck, but he now has a bit of ‘not pain, but an uncomfortable feeling’ in his upper back. You give him an additional dose of morphine 10 mg intravenously, in 2.5 mg aliquots, but it gives little relief. He becomes nauseous, and you administer ondansetron 4 mg intravenously.
The patient’s vital signs are taken again. His blood pressure is 143/82 (right arm) and 139/78 (left arm). His heart rate is 84bpm and there is no radioradial or radiofemoral delay. You perform a detailed physical examination and find no cardiovascular, respiratory, gastrointestinal or neurological abnormalities.
What investigations are required?
A mobile chest x-ray is performed and shows no abnormalities. Blood tests are ordered, which include: venous blood gas; full blood count; electrolytes, urea and creatinine; troponin; liver function tests; lipase and C-reactive protein. Repeat ECGs are performed every five minutes.
As the patient is in ongoing severe pain, you administer fentanyl 100 mcg intravenously. He says that the pain immediately improves, but he indicates that he now has a bit of epigastric pain. You perform a bedside point-of-care ultrasound of the upper abdomen, which shows no abnormalities including no gallstones, a normal sized aorta and no pericardial effusion. As his pain is much improved and the serial ECGs show no dynamic change, you decrease the frequency of ECGs – initially to every 15 minutes and then after one hour to another in three hours, with repeat troponin measurements. He still has discomfort in his chest and upper abdomen.
Given these findings, you keep a broad list of differential diagnoses in mind. These include acute myocardial infarction and upper abdominal conditions, including pancreatitis and peptic ulcer disease.
Results of the patient’s initial blood tests are returned and are largely within normal ranges. The only abnormalities are gamma glutamyltransferase 68 U/L (reference range [RR], <50 U/L) and white cell count 12.4x109/L (RR, 2-8 x109/L). In particular, his initial troponin level is 12 ng/L (RR, <14 ng/L), which suggests no major myocardial injury. You discuss his case with the cardiologist on call and admit him to the hospital for monitoring and a repeat troponin measurement.
What happens after admission?
After two hours, the patient’s severe pain returns with sharp radiation to his back, between his shoulder blades. He is again treated with intravenous fentanyl. An urgent CT aortogram is performed and shows a type A (Stanford classification) aortic dissection with a double lumen.
The patient is brought back to the resuscitation area and cardiothoracic and intensive care teams are immediately contacted. While waiting for transfer to theatre, he is treated with intravenous esmolol (500 mcg/kg over one minute, repeated every five minutes), and he is started on an esmolol infusion (50 mcg/kg/min) titrated to systolic blood pressure 100 to 110 mmHg. A second agent is needed to achieve the blood pressure targets, so a nitroprusside infusion (0.25 to 10 mcg/kg/min) is started after the esmolol infusion, to avoid the risk of reflex tachycardia. An arterial line is inserted for strict blood pressure monitoring.
During the operation an undiagnosed coarctation of the aorta is found. Fortunately, there is no rupture into the pericardium or dissection of the ostia of the coronary vessels and the patient recovers well postoperatively.
Discussion
Aortic dissection is a life-threatening diagnosis that is frequently missed, with potentially devastating outcomes. With this in mind, it is timely to review the features of a clinical presentation that are associated with a high risk of aortic dissection. Predisposing factors are presented in Box 1.1
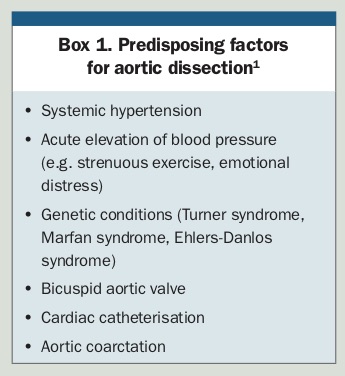{kind=link}
Accurate diagnosis of aortic dissection can be challenging because the symptoms and signs have low sensitivity and specificity. The condition is one of the great ‘masquerades’ – aortic dissection can mimic acute coronary syndrome, cerebral stroke, mesenteric bowel ischaemia, acute kidney injury and renal colic, as the dissection occludes the supply arteries to multiple organs.
There are many classic features of aortic dissection. These include:
- tearing pain
- new heart murmur
- migratory pain
- hypotension
- pulse deficit
- blood pressure differential in arms >20 mmHg
- symptoms above and below the diaphragm
- neurological signs.
Current literature suggests, however, that several classic signs are frequently absent and therefore less helpful in making a diagnosis. The clinical features associated with an increased likelihood of aortic dissection, which are listed in Box 2, are hypotension, pulse deficit, neurological deficit and new murmur.2 In addition, current evidence suggests that the absence of sudden pain that is maximal in intensity at onset is a negative predictive historical feature for aortic dissection.3
{kind=link}
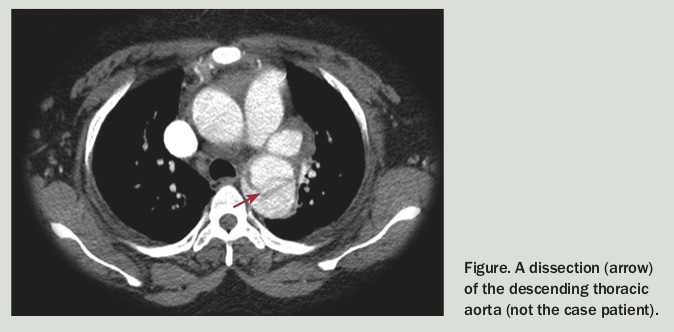
Multiple imaging modalities are considered for aortic dissection (Figure). However, when a patient is at high risk for aortic dissection, CT aortogram is the gold standard. A chest x-ray can be performed rapidly to exclude other diagnoses and, if performed, may reveal additional high-risk features (Box 3).4
{kind=link}
{kind=link}
Final comments
Aortic dissection is a crucial diagnosis that relies on suspicion but may not be straightforward. Interestingly, this case demonstrates why there is often uncertainty around the diagnosis. One feature that would suggest that aortic dissection is a less likely diagnosis is the lack of an abrupt onset of pain. Chest pain is a very common presenting symptom that requires a time-critical, thorough and suspicious approach to diagnosis – especially if the clinical picture is not clear or has distractors – to ensure several serious, at times life-threatening abnormalities are not missed. CT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.