Common causes of ST elevation

Myocardial infarction
ST elevation on an ECG can indicate acute ST elevation myocardial infarction (STEMI) and this should always be considered first. However, there are several other conditions that also elevate the ST segment and other features must be used to distinguish between them.
- The 12-lead ECG is an integral part of the diagnostic work up of a patient with acute chest pain.
- ST elevation in a 12-lead ECG is an important feature in the diagnosis and treatment of acute myocardial infarction (AMI).
- Several other clinical conditions can result in ST elevation.
- At times, distinguishing between ST elevation AMI (STEMI) from non-ischaemic causes of elevation of the ST segment is difficult.
- STEMI is typically con ned to a vascular territory and has a convex upward shape.
Picture credit: © Mhelm3011/iStockphoto.com Model used for illustrative purposes only
Case scenario
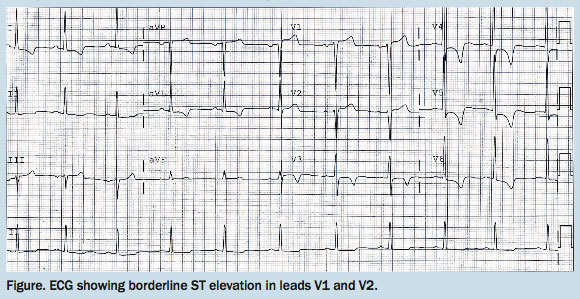
Olga, a 72-year-old previously well woman, felt lightheaded and experienced severe lower chest pain when at the shopping mall. First medical contact was made within 30 minutes and she was being treated at the nearby peripheral hospital within 45 minutes of onset of pain. On arrival, her blood pressure was 180/103 mmHg and she looked pale. An ECG (Figure) and troponin test were performed as part of her work up.
{kind=link}
Olga’s history included hypertension and hypercholesterolaemia, and she was a life-long smoker. She had no relevant family history and no previous cardiac events. She had recently travelled from interstate to look after her daughter who had had surgery.
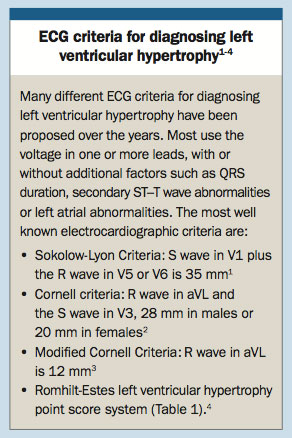
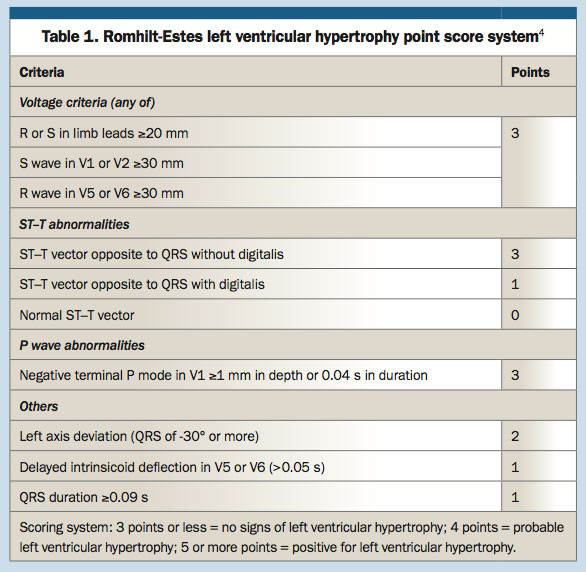
Olga’s ECG shows left ventricular hypertrophy (LVH; Box and Table 1).1-4 She had borderline ST elevation (<2 mm) in the anterior chest leads without any reciprocal ST depression in the inferior leads. A chest x-ray revealed a widened mediastinum and a CT aortogram showed a large dissection of the thoracic aorta. Olga was immediately transferred to the nearest tertiary hospital while continuing blood pressure-lowering treatment and adequate pain relief. Fortunately, Olga did not receive any thrombolysis, antiplatelet agents or heparin.
{kind=link}
{kind=link}
Commentary
Chest pain and other symptoms suggestive of acute coronary syndrome are among the most common reasons for patients seeking medical attention from their GPs or the hospital emergency department. The underlying cause of these presentations may range from minor disease such as musculoskeletal pain to life-threatening conditions such as acute myocardial infarction (AMI), aortic dissection or pulmonary embolism.
Patients with chest pain require a prompt diagnosis. This can be achieved by taking a focused history and conducting a clinical examination and basic investigations, including an ECG, a chest x-ray and blood tests. Failing to diagnose a life-threatening condition can result in mortality or serious morbidity for the patient, and also represents a frequent cause of malpractice cases.5
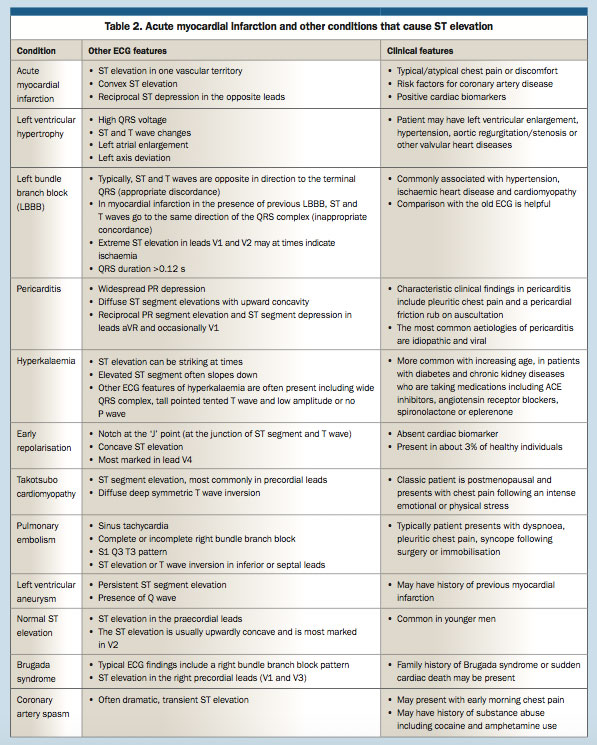
A delayed diagnosis of MI can mean that a patient misses the window of opportunity for immediate thrombolysis or primary angioplasty. ECG plays an important role in the early diagnosis of acute ST elevation MI (STEMI) before an immediate reperfusion strategy can be drawn. Although ST elevation in a standard 12-lead ECG is an important factor to consider in the treatment of MI, several clinical conditions result in ST elevation mimicking AMI (Table 2).
{kind=link}
In a US prospective observational study, it was found that in the emergency setting ST segment and T wave abnormalities were frequently misread, with 41% false negatives and 14% false positives.6 Although AMI needs to be considered first and foremost in the presence of ST elevation, it is not always the cause. A retrospective ECG review of adults with chest pain found only 15% of patients had STEMI and 85% of patients with ST elevation had a non-AMI diagnosis responsible for the ST elevation.7 Thrombolysis in the wrong clinical setting can result in catastrophic complications such as intracranial haemorrhage and death.
This article discusses common causes of ST elevation in the standard 12-lead ECG and ways to differentiate these conditions.
Acute myocardial infarction
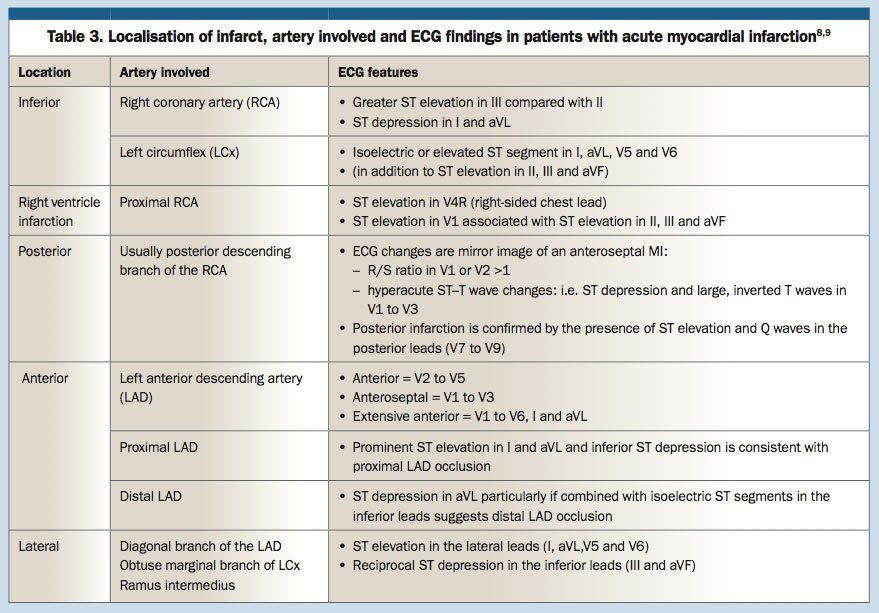
An ECG is considered to be an essential part of the evaluation of chest pain and diagnosis of AMI. Patients with typical ST elevation or new left bundle branch block (LBBB) are usually referred for immediate reperfusion therapy. An ECG in the setting of AMI can help localise the infarct, identify the coronary artery involved and predict the infarct size and prognosis.
STEMI is typically confined to a vascular territory, and the ST elevation has a convex upward shape (Table 3).8,9 Often there is reciprocal ST depression in the opposite leads. In the early stages of AMI, ECG may show a tall peaked T wave preceding the ST elevation. As the condition progresses, the ECG shows Q wave formation and T wave inversion.
{kind=link}
In the current Australian guidelines, the ECG criteria for the diagnosis of STEMI are development of new LBBB or persistent (>20 minutes) ST elevation in two or more contiguous leads of:10
- 2.5 mm ST elevation in leads V2 to V3 in men under 40 years
- 2 mm in V2 to V3 in men over 40 years
- 1.5 mm in V2 to V3 in women
- 1 mm in other leads.
Left ventricular hypertrophy
LVH is frequently associated with secondary ST segment or T wave abnormalities. The ST segment and T wave are directed opposite to the QRS complex: this is called discordance between the QRS complex and the ST–T abnormalities. That means there is typically ST elevation in the precordial leads VI and V2 (Figure), where the QRS complex is predominantly negative. In leads I, II, aVL, V4, V5 and V6, where the QRS complex is upright, the ST segment is often depressed (strain pattern).
ST elevation due to LVH is typically concave and is evident in addition to other features of LVH (Box).1-4 In a retrospective review of the ECGs from adults with chest pain presenting to an emergency department, LVH was found most often (25%) to be responsible for electrocardiographic ST elevation.7
Takotsubo cardiomyopathy
Takotsubo cardiomyopathy mimics AMI in presentation and should be considered in all postmenopausal women who present with chest pain after intense emotional or physical stress; however, about 20 to 35% of cases may not reveal any obvious precipitant. The patient may also present with dyspnoea, palpitations, syncope, cardiac arrest or ECG changes. Although a chest x-ray may be normal, the patient may present with acute pulmonary oedema and cardiomegaly.
The most common acute ECG findings of takotsubo cardiomyopathy are ST elevation in the precordial leads and T wave inversions in almost all leads.11 Unlike in AMI, ECG changes in takotsubo cardiomyopathy are not limited to one vascular territory. ECG findings are often dramatic and not in proportion with the changes in the patient’s troponin levels. Patients also may develop pathological Q waves that typically resolve before hospital discharge with restoration of normal R wave progression and prolonged QT interval (beginning of Q wave to end of T wave), which usually normalises in one to two days and prolonged PR (beginning of P wave to beginning of QRS complex) interval.12
The diffuse ST elevations that do not follow any vascular territory and the absence of reciprocal ST changes makes the diagnosis of STEMI unlikely. ST elevation in patients with myocardial infarction is reciprocal between leads III and aVL.
Pericarditis
In patients with acute pericarditis, the ST segment is elevated diffusely with upward concavity in the precordial and the limb leads. The ST elevation usually involves more than one coronary vascular territory and there is an absence of reciprocal ST changes between leads III and aVL. In patients with pericarditis, the PR segment is depressed but this is not specific for acute pericarditis as early repolarisation or atrial infarction can also cause the depression.13,14
Acute myocarditis can cause diffuse ST elevation similar to that seen in pericarditis. In Olga’s case, the absence of any systemic symptoms and absence of prior illness made the diagnosis of pericarditis or myocarditis unlikely.
Early repolarisation
Early repolarisation is characterised by ST elevation with a concave morphology and notching of the J point (the junction where the QRS complex ends and the ST segment begins). It is seen in leads with a tall R wave and is most marked in V4 (V2 to V5). Rarely, it can involve inferior leads.
It occurs in 2 to 5% of the population, predominantly in young men. Reciprocal changes typically seen in patients with AMI are generally absent. Unless associated with an acute coronary syndrome, the cardiac biomarker troponin should be negative.
Although sometimes called ‘benign early repolarisation’, whether it is a totally benign condition or carries slightly increased risk of sudden cardiac death remains controversial. A Finnish study found that patients with J-point elevation of more than 0.1 mV in inferior or lateral leads were about 1.3 times more likely to die from sudden cardiac death, whereas those who had J-point elevation of more than 0.2 mV were three times more likely to have sudden cardiac death.15 On the other hand, no significant association between any components of early repolarisation and cardiac mortality has been found.16
Normal ST elevation
A study of 6014 asymptomatic men, conducted to delineate the range of variation in a normal ECG, found that ST elevation in the precordial leads is very common (91.2%). ST elevation was most marked in the anterior leads (elevation in V2 to V4; 43.8%), followed by the lateral leads (elevation in V3 to V6; 24%), anterolateral leads (elevation in all precordial leads; 16.8%) and rightward (elevation in V1 to V2 only; 6.8%). Only 8.8% of men had no ST elevation in any precordial leads, 44.3% had 0.1 mV ST elevation, 38.4% had 0.2 mV ST elevation and 0.1% had ST elevation of 0.5 mV. The ST elevation is usually upwardly concave and is most marked in V2. ST elevation is common in younger men and the prevalence decreases with age.17
Left bundle branch block
The guidelines for the management of patients with AMI recommend immediate revascularisation with thrombolysis or primary angioplasty for patients with chest pain and new LBBB.10 ECG changes in the presence of pre-existing LBBB is slightly more complex because ST segment and T wave changes including ST elevation and ST depression in the presence of LBBB are common.10
Normally in LBBB, the ST segments and T waves are opposite in direction to the terminal QRS deflection. These changes are secondary to the bundle branch block (secondary ST segment and T wave changes). This means that in the presence of LBBB the septal leads (V1 to V3) quite often show ST elevation and an upright T wave where the QRS complex is predominantly negative. There is also association with ST depression and T wave inversion in the lateral leads (V5 and V6) where the QRS complex is predominantly positive. This is called ‘appropriate discordance’.
ST elevation in association with a positive QRS complex (in V4 to V6) or ST depression in leads that have predominantly negative QRS complexes (V1 to V3) is not expected in patients with uncomplicated LBBB and is termed ‘inappropriate concordance’, which strongly indicates the presence of acute ischaemia.
In patients with LBBB, the modified Sgarbossa criteria is useful in identifying STEMI: ST elevation of more than 1 mm concordant with QRS (five points); ST depression of more than 1 mm in lead V1 to V3 (three points); ST elevation more than 5 mm discordant with QRS (two points).10,18 More than three points is associated with a 98% chance of having MI, but a score of 0 does not rule out STEMI.
Hyperkalaemia
ST elevation in hyperkalaemia can be striking at times.19 Other ECG features of hyperkalaemia that can be present are widened QRS complexes; tall, pointed T waves and low amplitude or no P waves. In hyperkalaemia, the ST segment often slopes downward.
Hyperkalaemia is more common with increasing age and in patients with diabetes and chronic kidney disease who take medications that block the renin-angiotensin-aldosterone system including ACE inhibitors, angiotensin receptor blockers, direct renin inhibitors and aldosterone receptor antagonists such as spironolactone or eplerenone.
Left ventricular aneurysm
A left ventricular aneurysm can be diagnosed on ECG when there is persistent ST elevation with Q wave after a transmural myocardial infarction. In a patient with an anterior or apical aneurysm, the persistent ST elevation is most marked in lead V1 and V2. In a patient with an aneurysm after an inferior MI, changes are marked in leads II, III and aVF.20
The patient’s history of a previous AMI and an echocardiography is helpful to document the presence of an aneurysm. The shape of the ST elevation is also relatively unique and has been described as ‘coving’ (over Q waves).
Brugada syndrome
The Brugada syndrome is a familial disease with an autosomal dominant mode of transmission. Family history is often positive for sudden cardiac death at a young age, most commonly occurring during sleep, in particular during the early morning hours.21
Typical ECG findings of Brugada syndrome include a right bundle branch block (RBBB) pattern and ST elevation in the right praecordial leads (V1 and V3) in the absence of long QT intervals and any structural disease.22 The ST elevation can have a saddleback shape but in typical cases the ST segment is down sloping and ends with an inverted T wave. ST elevation in Brugada syndrome may be present intermittently. Challenging the patient with a sodium channel blocker such as flecainide can unmask a typical electrocardiographic pattern.23
Pulmonary embolism
ECG features of pulmonary embolism include sinus tachycardia, simultaneous T wave inversions in the inferior (II, III and aVF) and right precordial (V1 to V4) leads, ST elevation, S1 Q3 T3 pattern (deep S wave in lead I, Q wave in III, inverted T wave in III) and complete or incomplete RBBB. ST elevation in the presence of massive pulmonary embolism can be striking at times.24
Consider pulmonary embolism as a differential diagnosis in any patient who presents with chest pain, dyspnoea and syncope in the postoperative setting or after prolonged immobilisation. Patients may have an elevated jugular venous pressure and other signs of congestive cardiac failure. A D-dimer test is very helpful in excluding pulmonary embolism as it is considered a highly sensitive test for pulmonary embolism and a negative test makes diagnosis of pulmonary embolism unlikely. Unfortunately, D-dimer lacks specificity and has low positive predictive value. When clinical suspicion of pulmonary embolism is high, a CT pulmonary angiogram may be needed to confirm the diagnosis.
Coronary artery spasm
Spasm of an epicardial coronary artery can produce dramatic, transient ST elevation in patients with chest pain. Although coronary spasm is usually brief and the ST segment returns to normal without myocardial injury, prolonged spasm can result in MI.25 Vagal withdrawal is most often the mechanism leading to spontaneous spasm.
Patients with coronary artery spasm are usually younger than those that present with unstable angina or chronic stable angina and tend to present with early morning chest pain. An important associated risk factor is substance abuse including tobacco and marijuana smoking, alcohol consumption and cocaine and amphetamine use.
Conclusion
The 12-lead ECG is an integral part of the diagnostic work up of a patient with acute chest pain. It is the recommended bedside test to confirm or exclude the diagnosis of STEMI and AMI needs to be considered first and foremost.
ST elevation caused by conditions other than acute ischaemia is common. At times, distinguishing between STEMI from nonischaemic causes of elevation of the ST segment is difficult, especially in patients with atypical presenting symptoms. Understanding common patterns of ST elevation that are not caused by ischaemia is crucial for rapid and accurate diagnosis of STEMI and subsequent reperfusion strategy.
In a certain clinical context, when equivocal ECG abnormalities are detected, other differential diagnoses should be taken into account in order to avoid unnecessary, potentially dangerous therapies. Serial ECG, comparison to old ECGs, ST elevation confined to single vascular territories with or without reciprocal ST depression, expert help and at times remote ECG review can assist in the diagnosis of STEMI.
References
- Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J 1949; 37: 161-186.
- Casale PN, Devereux RB, Kligfield P, et al. Electrocardiographic detection of left ventricular hypertrophy: development and prospective validation of improved criteria. J Am Coll Cardiol 1985; 6: 572-580.
- Molloy TJ, Okin PM, Devereux RB, Kligfield P. Electrocardiographic detection of left ventricular hypertrophy by the simple QRS voltage-duration product. J Am Coll Cardiol 1992; 20: 1180-1186.
- Romhilt DW, Estes EH Jr. A point-score system for the ECG diagnosis of left ventricular hypertrophy. Am Heart J 1968; 75: 752-758.
- Rusnak RA, Stair TO, Hansen K, et al. Litigation against the emergency physician: common features in cases of missed myocardial infarction. Ann Emerg Med 1989; 18: 1029-1034.
- Jayes RL, Larsen GC, Beshansky JR, D’Agostino RB, Selker HP. Physician electrocardiogram reading in the emergency department - accuracy and effect on triage decisions: findings from a multicenter study. J Gen Intern Med 1992; 7: 387-392.
- Brady WJ, Perron AD, Martin ML, Beagle C, Aufderheide TP. Cause of ST segment abnormality in ED chest pain patients. Am J Emerg Med 2001; 19: 25-28.
- Zimetbaum PJ, Josephson ME. Use of the electrocardiogram in acute myocardial infarction. N Engl J Med 2003; 348: 933-940.
- Arbane M, Goy JJ. Prediction of the site of total occlusion in the left anterior descending coronary artery using admission electrocardiogram in anterior wall acute myocardial infarction. Am J Cardiol 2000; 85: 487-491.
- Chew DP, Scott IA, Cullen L, et al. National Heart Foundation of Australia & Cardiac Society of Australia and New Zealand: Australian clinical guidelines for the management of acute coronary syndromes 2016. Heart Lung Circ 2016; 25: 895-951.
- Rahman A, Liu D. Broken heart syndrome: a case study. Aust Fam Physician 2012; 41: 55-58.
- Bybee KA, Kara T, Prasad A, et al. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med 2004; 141: 858-865.
- Spodick DH. Diagnostic electrocardiographic sequences in acute pericarditis: significance of PR segment and PR vector changes. Circulation 1973; 48: 575-580.
- Rahman A, Liu D. Pericarditis: clinical features and management. Aust Fam Physician 2011; 40: 791-796.
- Tikkanen JT, Anttonen O, Junttila MJ, et al. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med 2009; 361: 2529-2537.
- Uberoi A, Jain NA, Perez M, et al. Early repolarization in an ambulatory clinical population. Circulation 2011; 124: 2208-2214.
- Hiss RG, Lamb LE, Allen MF. Electrocardiographic findings in 67,375 asymptomatic subjects. Am J Cardiol 1960; 6: 200-231.
- Sgarbossa EB, Pinski SL, Barbagelata A, Underwood DA, Gates KB, Topol EJ. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. N Engl J Med 1996; 334: 481-487.
- Sims DB, Sperling LS. Images in cardiovascular medicine. ST-segment elevation resulting from hyperkalemia. Circulation 2005; 111: e295-e296.
- Smith SW. T/QRS ratio best distinguishes ventricular aneurysm from anterior myocardial infarction. Am J Emerg Med 2005; 23: 279-287.
- Matsuo K, Kurita T, Inagaki M, et al. The circadian pattern of the development of ventricular fibrillation in patients with Brugada syndrome. Eur Heart J 1999; 20: 465-470.
- Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sudden cardiac death: a distinct clinical and electrocardiographic syndrome: a multicenter report. J Am Coll Cardiol 1992; 20: 1391-1396.
- Brugada R, Brugada J, Antzelevitch C, et al. Sodium channel blockers identify risk for sudden death in patients with ST-segment elevation and right bundle branch block but structurally normal hearts. Circulation 2000; 101: 510-515.
- Wang K, Asinger RW, Marriott HJ. ST-segment elevation in conditions other than acute myocardial infarction. N Engl J Med 2003; 349: 2128-2135.
-
Stern S, Bayes de Luna A. Coronary artery spasm: a 2009 update. Circulation 2009; 119: 2531-2534.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.