New guidelines for cardiovascular genetic testing: what the GP needs to know

Cardiac genetic testing is a rapidly growing area, with increasing availability, reducing costs and improved understanding of the importance of comprehensive management for patients and families with inherited cardiovascular diseases. However, interpretation of genetic results is complex, requiring specialised multidisciplinary input. GPs have a multifaceted role in managing patients with genetic heart disease and their families, especially after an unexplained sudden death.
- Cardiac genetic testing has rapidly emerged, is increasingly available and is now becoming part of standard clinical cardiology practice.
- The interpretation of genetic test results is complex, requiring specialised multidisciplinary input.
- Before a person undergoes genetic testing, they should have a detailed three-generational family history taken and undergo pre-test genetic counselling; after testing, they should have post-test genetic counselling to discuss their results.
- Targeted panel genetic testing for genes is usually preferred rather than larger whole exome or genome sequencing in the first instance.
- There are important potential benefits to proceeding with cardiac genetic testing including being able to offer predictive testing to first-degree family members; informing reproductive choices; and guiding diagnostic, therapeutic and prognostic decisions.
- GPs are an integral part of the multidisciplinary team providing care for individuals and families with inherited cardiovascular diseases or after an unexplained sudden death.
Cardiac genetic testing and its utility in patients with inherited cardiovascular diseases (CVDs) have evolved considerably over the past 10 to 15 years and continues to be a rapidly advancing field. Over this time there has been considerable progress in our understanding of the genetic basis of disease, and, therefore, the widespread utility of genetic testing in terms of improving diagnosis, guiding management decisions and informing prognosis for patients and families. This has come in conjunction with reduced costs and improved access to genetic testing, meaning that genetic testing is now becoming more widely available to the population. However, genetic testing is complex, with interpretation of variants and genotype-phenotype correlation (i.e. understanding how the gene causes disease in the individual) requiring specialised multidisciplinary input. There are important practical considerations before embarking on cardiac genetic testing.
This article aims to highlight key considerations from the recently published international cardiovascular genetic testing guidelines for GPs and general cardiologists to help with understanding, performing and interpreting cardiac genetic testing in patients with inherited CVDs and their families.1
The cardiac genetic testing process
When to consider genetic testing
Genetic testing should be considered in an individual after comprehensive cardiac phenotyping has identified a diagnosis or highly suspected genetic cardiac condition. Cardiac phenotyping usually involves an electrocardiogram, echocardiogram, 24-hour Holter monitor with or without exercise stress testing, and cardiac MRI. Genetic testing is not usually indicated before detailed cardiac investigations when assessing these patients.
Before proceeding with genetic testing, taking a detailed three-generational family history is essential. If the phenotyping and family history suggest an inherited basis to disease, then genetic testing is usually indicated, or at least considered. In some individuals with no family history, genetic testing may also be indicated on a case-by-case basis.
Pre-test counselling
It is important that the individual undergoes pre-test genetic counselling by a trained genetic counsellor or a cardiologist/clinical geneticist experienced in cardiac genetics. Genetic testing results are not binary (yes/no), but rather there is a spectrum of pathogenicity with a probabilistic outcome as the final result. The individual being tested needs to understand the potential for uncertainty with genetic testing, particularly in the case of identification of variants of uncertain significance.2 To ensure that accurate information is portrayed to patients and families, and particularly given the challenges of variant interpretation, it is generally recommended that only genes that have an established basis for disease are tested.1
Establishing the pathogenicity of a variant
Genetic testing results are reviewed by scientists and genetic counsellors at the laboratory performing the testing, often as part of a multidisciplinary meeting. The process of establishing pathogenicity is determined by a composite of criteria including the following:
- the variant being rare in general population databases
- whether the variant has previously been associated with the disease in question
- whether the variant is predicted to cause effects on the function of the protein
- whether there are cell or animal data to suggest effects on the protein function.
These criteria have been published by the American College of Medical Genetics and Genomics, and only those variants that are classified as pathogenic (P) or likely pathogenic (LP) according to these criteria are considered to be causal of disease.3 Benign (B) and likely benign (LB) variants are considered negative results. Variants of uncertain significance are unable to be further classified as either causal or negative without more information.
Post-test counselling
When the variant’s pathogenicity has been confirmed, results are then fed back to the individual by specialised cardiac genetic counsellors or a cardiologist/clinical geneticist experienced in cardiac genetics, with post-test genetic counselling occurring at this time. It is important to note that uncertain genetic testing results are reviewed and reappraised in time, and potentially reclassified, as new knowledge and research are established.
The Flowchart summarises the cardiac genetic testing processes for an individual suspected of having a genetic cardiac disease.
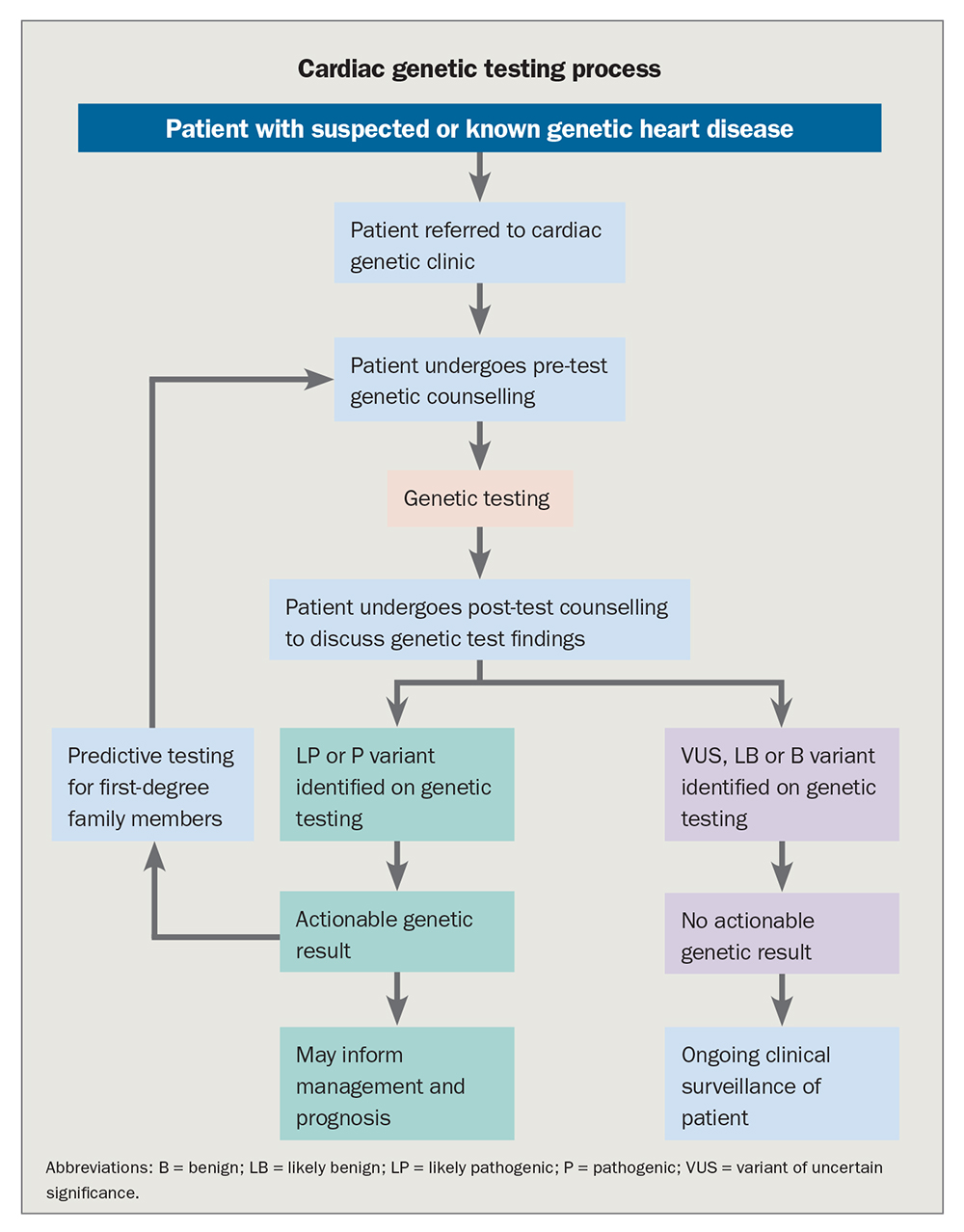{kind=link}
MBS item numbers
There are now new Medicare Benefits Schedule (MBS) item numbers with strict eligibility criteria for once-off cardiac genetic testing for individuals for whom clinical or family history is suggestive of an inherited arrhythmia syndrome or inherited cardiomyopathy. These individuals are best referred to a specialised multidisciplinary clinic for assessment and review of eligibility/appropriateness.
Once a genetic cause is identified in an individual, MBS item numbers are also now available for predictive (also known as cascade) genetic testing in at-risk relatives. Relatively new MBS item numbers are also available for once-off testing for familial hyperlipidaemia (FH) with strict eligibility requirements for total cholesterol and low density lipoprotein levels or Dutch Lipid network scores that need to be documented at the time of ordering the test.
Cardiac diseases that should be considered for genetic testing
Several CVDs have been clearly established to have a genetic basis, whereby genetic testing can be considered. The diseases for which genetic testing is most useful are those with typical ‘Mendelian-type’ inheritance whereby ultrarare genetic changes can have a large effect size (and thereby lead to disease).2 These include the following:
- the cardiomyopathies – including hypertrophic cardiomyopathy (HCM), arrhythmogenic (right ventricular) cardiomyopathy (ACM/ARVC), dilated cardiomyopathy (DCM) and left ventricular noncompaction cardiomyopathy (LVNC)
- the channelopathies – including long QT syndrome (LQTS), Brugada syndrome (BrS), catecholaminergic polymorphic ventricular tachycardia (CPVT), short QT syndrome (SQTS) and progressive cardiac conduction disease (PCCD).
Other cardiac conditions whereby genetic testing can be useful include FH, genetic aortopathies (e.g. Marfan syndrome or familial thoracic aortic aneurysm and dissection [TAAD]) and inherited congenital disease (e.g. Holt-Oram syndrome).
Genetic testing may also be indicated after sudden death or sudden cardiac arrest in a young person aged under 35 years, including both targeted testing when autopsy suggests a diagnosis of an inherited condition (e.g. HCM) or broader channelopathy and cardiomyopathy panel testing when the autopsy results are unexplained. In all sudden cardiac death cases in the young, a 5 to 10 mL blood sample should be collected for subsequent DNA extraction and analysis. In addition, frozen sections of liver or spleen (which are rich in DNA) can be collected and stored. In cases of sudden death where no cause is identified after a complete and thorough postmortem examination, genetic testing of the decedent’s blood sample (postmortem genetic testing) may identify an underlying cause for the unexplained death.
In most inherited CVDs, the yield of testing is higher in individuals who have a family history of disease. The highest yield for genetic testing in the channelopathies is in LQTS (about 70%), with the lowest yield in BrS (about 10 to 20%). In the cardiomyopathies, the highest yield is in HCM and ACM (about 50%), whereas the lowest yield is in LVNC (about 5 to 10%).
It is often tempting to order a larger genetic panel encompassing ‘more genes to yield more results’; however, multiple studies have shown that the diagnostic utility is not increased when genes that do not have strong evidence for disease-causation are incorporated into the testing panel. In such cases, the yield of variants of uncertain significance is increased, potentially adding further uncertainty to the results.4
The ClinGen initiative has recently reviewed the evidence for causality and genotype-phenotype associations for several inherited cardiac conditions, with the published documents providing an evidence-based reference tool for clinicians and scientists to review when considering genetic testing results.5 Therefore, our current recommendation is to order targeted panel genetic testing for genes that are known to be associated with the disease in question. Further broad exome or genome sequencing can potentially be offered as part of a research setting when standard cardiac panel testing has failed to identify an established genetic cause of disease.
The Table lists some important do’s and don’ts of cardiac genetic testing.
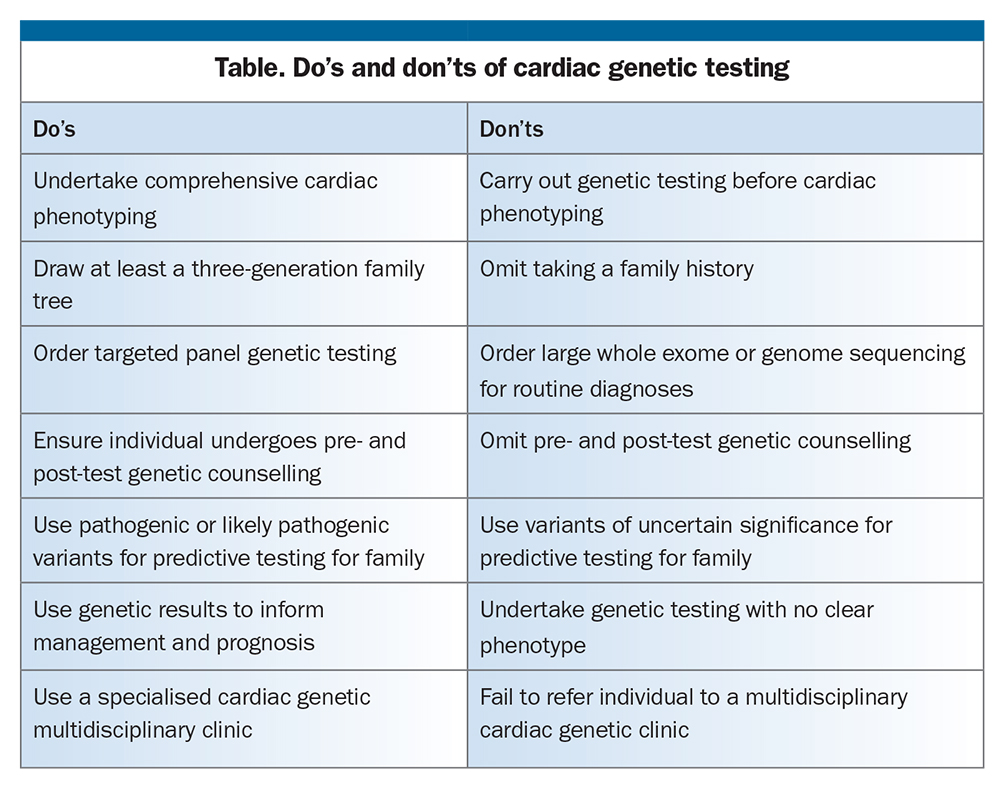{kind=link}
Clinical impact of cardiac genetic testing
Offering predictive testing to first-degree relatives
The greatest utility for genetic testing is in offering predictive testing to first-degree family members in the case of LP or P results. Most monogenic CVDs are inherited in an autosomal dominant manner, meaning first-degree relatives have a 50% chance of carrying the same variant.6 For any family member who is subsequently found to carry the variant, then their first-degree relatives should also be offered testing and counselling, and this process continues until all extended at-risk family members have been offered clinical screening and genetic testing. Some family members may choose not to undergo predictive genetic testing; these individuals should continue regular clinical screening and ongoing surveillance with a cardiologist. Predictive testing is not recommended or indicated with variants of uncertain significance.
Informing reproductive decisions
Positive genetic results (P or LP) can also inform reproductive decisions for patients and families. For example, a positive gene result can be used in prenatal genetic testing to facilitate preimplantation genetic diagnosis whereby embryos from IVF found to carry the causative variant are not implanted. This ensures the future child is not at risk for the particular inherited CVD.
Guiding diagnostic, therapeutic and prognostic decisions
Genetic testing also has diagnostic, therapeutic and prognostic utility depending on the disease in question. ACM is an important cause of sudden cardiac death in athletes due to ventricular arrhythmias provoked by exercise. In ACM, individuals carrying a pathogenic genetic variant have a greater chance of progression to overt disease, heart failure and life-threatening arrhythmias with high-level athletic activity, even in the absence of any evidence of cardiomyopathy. Therefore exercise restriction is recommended in these individuals.7-9 Predictive genetic testing is integral in managing families with ACM to identify those individuals within the family who are genotype-positive who may not yet show evidence of disease, in whom it is still recommended to avoid competitive sports.8
In LQTS, the genotype can help with diagnosis, prognosis and management decisions. There are known specific genotype-associated triggers for arrhythmia, including strenuous exercise, particularly swimming (LQT1), loud noise/alarm clocks (LQT2) and sleep (LQT3).10 These can guide lifestyle recommendations for individuals who are genotype positive. Genetic testing helps in evaluating the prognosis for patients with LQTS, as their treating cardiologist can estimate their overall risk through a composite of the genotype and the QTc.11
Following an unexplained sudden death of an individual, identification of an underlying cause (through genetic testing) has major implications for surviving relatives, as well as giving the family some closure as to why their relative has died suddenly at a young age. Predictive testing in family members aims to identify those who may carry the same pathogenic variant as the decedent, even before they may show clinical evidence of disease. Early identification of these at-risk individuals provides opportunities to initiate therapies aimed at preventing the complications and ultimately aiming to prevent a further sudden death in the family. For example, gene carriers for LQTS may require modification of lifestyle activities, avoidance of QT-prolonging medications, initiation of beta-blocker therapy and, in some, consideration of implantable cardioverter defibrillator therapy.12
The role of the GP
As primary care physicians, GPs have a multifaceted role in managing patients with genetic heart disease and their families. They have an important role in educating patients on the increased availability and reduced cost of genetic testing (including MBS item numbers now available for cardiomyopathies, inherited arrhythmia syndromes and FH), taking a detailed family history, and navigating any difficult family dynamics, particularly in the circumstances of communication breakdown in families.
GPs are also key in identifying families for whom genetic testing may be useful, referring them to specialised cardiac genetics services for further assessment and management, and, finally, providing them with psychological support and linking them with allied health support services when needed. More information on referring patients to specialised cardiac genetic services is available at: http://www.heartregistry.org.au/patients-families/cardiac-genetic-services/.
Other areas where the role of the GP is of great importance include helping with medication adherence, ensuring the avoidance of medications such as QT-prolonging drugs, encouraging healthy lifestyle activities and addressing potential psychological issues such as guilt in families when a disease-causing variant is passed on. The GP is therefore an integral part of the multidisciplinary team providing care for individuals and families with inherited CVDs (Figure).
{kind=link}
Conclusion
Cardiac genetic testing has rapidly emerged, is more widely available and is now becoming part of standard clinical cardiology practice. It is critical that clinicians who are ordering genetic testing understand its utility and limitations and that any uncertain genetic testing results are reviewed over time and reappraised as new information is gathered. It is also important that appropriate pre- and post-test genetic counselling accompany all cardiac genetic testing so that the patient and their families understand fully the implications of testing. Therefore, genetic testing should be performed in the setting of a multidisciplinary cardiac genetic clinic. CT
COMPETING INTERESTS. Dr Gray has been an Advisory Board participant for Bristol Myers Squibb. Professor Semsarian: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.