Iron deficiency in heart failure: more than just fatigue

Heart failure
About half of patients with heart failure (HF) have iron deficiency (ID), which can occur without anaemia and can cause exacerbated symptoms and increased hospitalisation and mortality. Intravenous iron therapy improves symptoms and quality of life, and may improve survival in patients with HF and ID.
- Iron deficiency (ID) in heart failure (HF) is common and under-diagnosed.
- ID in patients with HF is not necessarily related to anaemia.
- ID causes increasing dyspnoea, deterioration in exercise capacity, fatigue, worse left ventricular function, higher rates of hospitalisation and increased mortality in patients with HF.
- Oral and intramuscular iron have no evidence of benefit in treating patients with HF and ID and are not recommended.
- Intravenous infusion of ferric carboxymaltose in patients with HF and ID can improve exercise capacity, quality of life, left ventricular function and may reduce HF hospitalisations and possibly improve survival.
Almost half a million (480,000) people in Australia have heart failure (HF). This equates to 6.3% of people aged 45 years or over, or more than 2.1% of the Australian population.1 An additional 30,000 cases are diagnosed each year.2 The annual cost of managing HF in Australia is almost $2.7 billion. In 2014, there were 27,468 hospital admissions for HF, of which 60% were admitted with a primary diagnosis of HF.1 HF also accounts for 3 to 4% of general practice consultations.3 Despite advances in therapy, the five-year mortality from HF is more than 50%.4
Iron deficiency (ID) affects about two billion people worldwide, and in developed countries it is estimated to involve 2% of men and 9% of women.5,6 ID is now recognised as a marker of adverse outcomes in HF and a therapeutic target in patients with HF.7 ID can occur without anaemia. The adverse effects and potential benefits of intravenous iron therapy go beyond those with low haemoglobin,8 including cellular, mitochondrial and muscle function, as well as reproduction of cells with high turnover.
Iron is crucial for the function of every cell in the body as it is an essential component of respiratory chain proteins in mitochondria and for energy generation (Figure 1).9 ID in patients with HF is associated with increased fatigue, breathlessness on exertion, reduced exercise capacity, poorer quality of life, worse symptoms of HF, higher rates of hospitalisation and increased mortality.7-10 These adverse effects are independent of anaemia in patients with HF and ID. Anaemia does not affect these adverse outcomes in HF when corrected for ID and other prognostic markers, although patients with both ID and anaemia have worse outcomes.7-10
{kind=link}
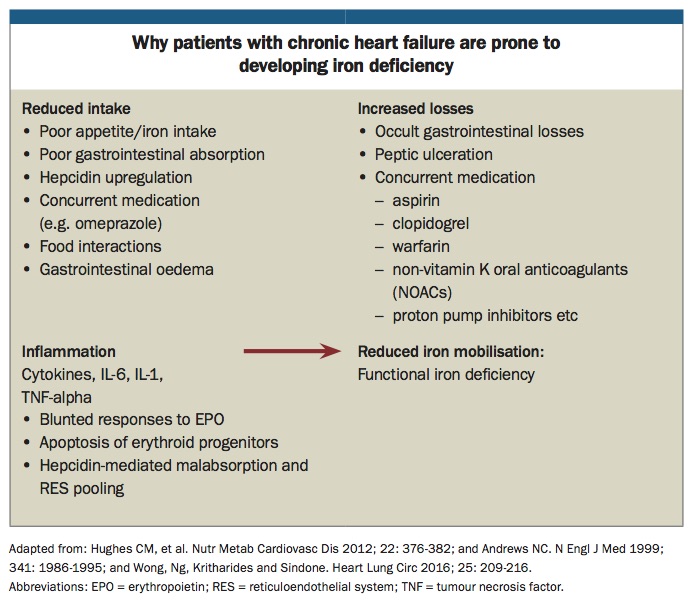
Why do patients with heart failure develop iron deficiency?
Ferrous iron (Fe2+) is absorbed in the proximal small bowel and exported by ferroportin to the blood where it is oxidised to ferric iron (Fe3+) and bound to transferrin. This complex is taken up by the spleen, bone marrow and liver in the form of ferritin.10 Patients with HF, which is a chronic inflammatory condition, have a high level of hydroxyl molecules (OH-) in the wall of their intestine, which may inhibit absorption of ferrous iron or conversion to ferric iron. Factors in patients with HF that may cause ID include reduced appetite, oedema of the bowel affecting iron absorption, co-administration of proton pump inhibitors and occult gastrointestinal blood loss (Box).11
{kind=link}
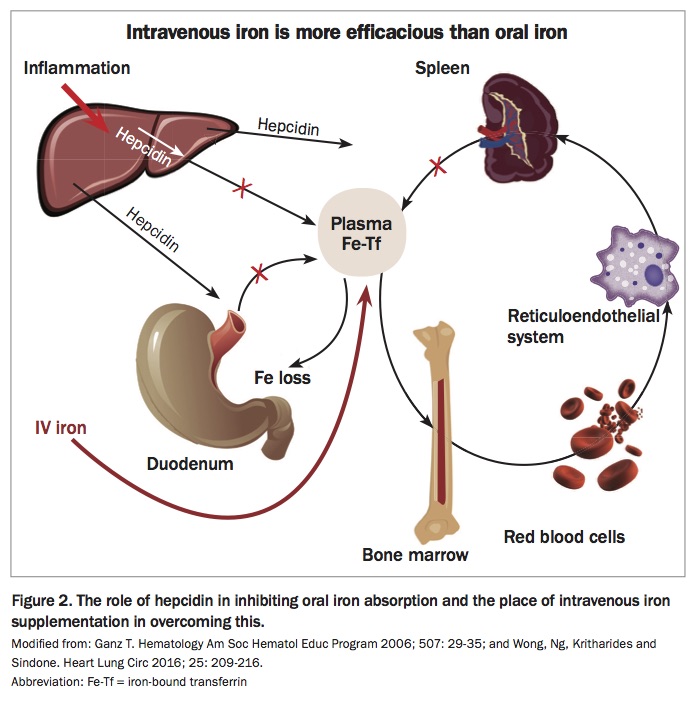
Patients with HF may also have high levels of hepcidin, which inhibits iron absorption by binding to ferroportin causing iron sequestration in the reticuloendothelial system and reducing the availability of useable iron (Figure 2).12
{kind=link}
Evaluation of iron deficiency in patients with heart failure
Iron status in patients with HF is routinely measured by measuring plasma ferritin, which is an indicator of iron stores. Patients with HF are diagnosed to have ID at ferritin levels of less than 100mcg/L.13 Ferritin levels may rise during acute illness as it is an acute phase reactant and HF is a chronic disease accompanied by inflammation. This is the reason the level of ferritin in patients with HF and ID is defined as less than 100mcg/L.14
Patients with low transferrin saturation (TSAT) have functional ID due to the reduced availability of iron for muscle and metabolic function; there may be insufficient iron stores for release into the circulation or because the iron is bound to ferroportin by hepcidin and cannot be released to the tissues where it is needed.15 Patients with HF who have a ferritin level of 100 to 300mcg/L and TSAT less than 20% are also classified as having ID (Figure 3).16 When these patients are treated with intravenous ferric carboxymaltose (FCM), there is a significant improvement in functional capacity, symptoms and quality of life.17
{kind=link}
ID without anaemia does not necessarily require investigation for the cause of ID unless there is absolute ID (ferritin <30mcg/L) or anaemia is also present.8 Causes of ID anaemia that may need to be excluded in such cases include: blood loss (particularly occult gastrointestinal bleeding); aspirin or NSAID use; reduced iron intake or absorption; or haematological, renal or liver disease.8
How common is iron deficiency in patients with heart failure?
About half of all patients with HF have ID. Studies have reported rates of 36 to 73%; prevalence increases with the severity of the HF and in the presence of anaemia.18 Australian data reflect this, with patients with HF and ID more likely to be female and to have a higher incidence of left ventricular dysfunction, worse renal function, advanced age, ischaemic heart disease, persistent tachycardia, and reduced ability to tolerate prognostically important medications for HF such as beta blockers and drugs that act on the renin-angiotensin system.19 The incidence of ID in patients with HF with preserved left ventricular ejection fraction (LVEF) may be slightly lower and is more closely related to symptoms and comorbidities.19
It is important to recognise that patients with HF do not have to have anaemia to have ID.20 ID is the most common cause of anaemia in patients with HF but may only account for 73% of cases, with the remainder due to haematological disorders.21 Conversely, ID may be present in about 32% of patients with HF in the absence of anaemia, again with the incidence rising proportionately with the severity of HF and comorbidities.20
Treatment of iron deficiency in patients with heart failure
Several studies of the effects of intravenous iron therapy in patients with HF and ID have shown improvements in exercise capacity, peak oxygen consumption on cardiopulmonary exercise testing, New York Heart Association (NYHA) functional classification of HF severity, quality of life assessments, elevated natriuretic hormones and left ventricular function in selected patients.22-27
Two landmark multicentre, international, double-blind, placebo-controlled trials of FCM changed the landscape of the management of ID in patients with HF. The FAIR-HF study randomised 459 patients with HF (NYHA II-III and LVEF ≤45%) and ID (ferritin <100ng/mL or ferritin 100 to 300ng/mL with TSAT <20% and haemoglobin 9.5 to 13.5g/dL) to FCM or placebo. At 24 weeks follow up, FCM treatment was associated with a significant improvement in Patient Global Assessment (PGA), NYHA class, distanced walked in a six-minute walk test and health-related quality of life (all p<0.001), and there was no difference in patients who also had anaemia (haemoglobin <120g/dL). There was also a non-significant trend towards reduced cardiovascular (CV) hospitalisation with no significant difference in adverse reactions to FCM therapy.17
The CONFIRM-HF study randomised 304 patients with HF (NYHA II-III and LVEF ≤45%, brain natriuretic peptide [BNP] >100pg/mL or NT-proBNP >400pg/mL) and ID (ferritin <100ng/mL or ferritin 100 to 300ng/mL with TSAT <20% and haemoglobin <15g/dL) to FCM or placebo.22 After 24 weeks of follow up, patients treated with FCM had significant improvements in six-minute walk test distance, PGA, NYHA class and health-related quality of life, which all remained improved to 52 weeks follow up. There was also a significant reduction in first hospitalisation for worsening HF or all-cause mortality, with no significant difference in adverse reactions to FCM therapy.22
The CONFIRM-HF study differed from the FAIR-HF study in that patients were administered up to 1000 mg FCM or placebo via 15-minute infusion or undiluted bolus over one minute in CONFIRM-HF and further doses were administered at 12, 24 and 36 weeks if ID was still present. This protocol is now recommended in treatment algorithms.17,22,28 The FAIR-HF study administered 200mg FCM or placebo once a week until the iron studies had normalised and then once a month until week 24.17
An individual patient data meta-analysis of four trials of intravenous iron therapy compared with placebo in 839 patients with HF (LVEF ≤45%) and ID showed a significant reduction in:
- recurrent cardiovascular hospitalisations and CV mortality by 41% (p= 0.009)
- recurrent HF hospitalisations and CV mortality by 47% (p=0.011)
- all-cause mortality by 40% (p=0.009).29
Although these data are robust and compelling, a large study of morbidity and mortality is underway to confirm this meta-analysis.30
Oral iron supplements have not been found to be effective in improving symptoms, quality of life or exercise capacity in patients with HF and ID in similar cohorts to those who have been shown to benefit from intravenous iron infusions in the recent large IRONOUT-HF trial and for this reason are not recommended in patients with HF and ID.31 There are no data regarding intramuscular iron injections in patients with HF and ID and it is not recommended in these patients. In fact, intravenous iron infusions may show some small improvements in quality of life after only a few days to one week.32
The 2016 European Society of Cardiology ‘Guidelines for the diagnosis and treatment of acute and chronic HF’, based on the above evidence, recommend ‘consideration of IV iron therapy in symptomatic patients with HFrEF [HF with reduced ejection fraction] and absolute or functional ID (serum ferritin <100 mcg/L, or ferritin 100 to 299 mcg/L and TSAT <20%) to alleviate HF symptoms and improve exercise capacity and quality of life’ regardless of the haemoglobin level (class of recommendation IIa, level of evidence A).33
Safety of iron infusions
Originally iron infusions were given as iron oxyhydroxide complex, which was associated with nausea, hypotension and peripheral oedema.34 Modern preparations contain an iron core surrounded by a carbohydrate shell, which has been found to minimise adverse reactions.34 FCM is the most studied iron preparation used in patients with HF. It is a very stable iron compound with slow degradation that can be safely given in a single, high-dose infusion.17,22,35 FCM does not require a test dose because it does not react with antidextran antibodies. Serum iron concentration increases rapidly after a single dose of FCM with distribution to the bone marrow, liver and spleen within 10 minutes.36
Adverse reactions, which are uncommon and usually transient, include:36
- mild but transient fall in serum phosphate (27%)
- true hypophosphataemia (2%)
- nausea (7%)
- hypertension (4%)
- flushing (4%)
- allergic reactions, which are reported to occur in 0.1% of cases.
Patients should be monitored for 30 minutes after administration of FCM in case of allergic reaction.36 Great care should be taken to avoid extravasation when administering FCM because leakage may result in long-term brown discolouration of the skin and irritation.37 If extravasation occurs, stop administration immediately.37 FCM is an easily administered and safe form of iron replacement in patients with HF and ID provided that infusions are carefully monitored and patients are observed for 30 minutes after completion of the infusion.
Conclusion
Iron is a critical component of cellular and muscular function, including cardiac muscle. ID in HF is relatively common and its effects are beyond anaemia. Patients with HF who have ID are more symptomatic and have a worse prognosis. Intravenous iron supplementation in patients with HF and ID is safe and improves symptoms, exercise capacity and quality of life. The effect of iron infusions on survival in patients with HF and ID is being investigated. CT
References
Chronic_Heart_Failure_Guidelines_2011.pdf (accessed May 2018).