Sudden cardiac death. Recognising and mitigating the risk

Cardiac arrest
Coronary artery disease
Sudden cardiac death is a significant source of mortality in the Australian population, most commonly related to underlying coronary artery disease. Early recognition of at-risk patients is key to preventing this catastrophic event.
- Sudden cardiac death (SCD) is defined as death due to a cardiac cause that occurs suddenly and unexpectedly if witnessed, or an unexpected death from a likely cardiac cause where the individual was known to be alive within the previous 24 hours.
- The most common cause of SCD is underlying coronary artery disease such as a previous myocardial infarction.
- Although patients with underlying heart disease have the highest rate of SCD, most absolute events occur in the general population without known heart disease.
- Investigations include blood biochemistry, electrocardiography and echocardiography.
- Management is often with beta blockers and, in high-risk patients or those with previous cardiac arrest or ventricular tachycardia, an implantable cardiac defibrillator.
Sudden cardiac death (SCD) is defined as death due to a cardiac cause that occurs suddenly and unexpectedly if witnessed, or an unexpected death from a cardiac cause where the individual was known to be alive within the previous 24 hours. SCD is one of the most common causes of death in Australia and is responsible for almost half of all deaths from cardiovascular disease.1 Despite significant improvements in treatment of heart disease, SCD occurrence, as a proportion of overall cardiac deaths, has increased. Cardiac arrest is a precursor to SCD, with similar underlying causes.Unfortunately, survival after an out-of-hospital cardiac arrest remains low, at only 12% at 30 days.2 It is therefore critical to ensure patients are receiving the right tests and care to prevent cardiac arrest and SCD.
The rate of SCD is greatly increased in high-risk individuals.3 People at high risk include survivors of cardiac arrest, patients who have suffered a myocardial infarction (MI) and patients with heart failure, especially those with a left ventricular ejection fraction (LVEF) less than 35%. However, a significant number of absolute events of sudden death still occur in the general population and in other high-risk patient populations, such as those with congenital heart disease.3
The key roles for the GP in the prevention of SCD include identifying at-risk patients and families who should be referred for cardiac assessment and providing long-term clinical and psychosocial care for families who have experienced SCD. The GP may also be the first to recognise the possibility of a genetic heart disease in an individual or in the family history. The GP is at the forefront with regard to SCD in the community and is an integral member of the multidisciplinary team caring for families affected by SCD and survivors of cardiac arrest.4
What causes sudden cardiac death?
SCD is usually due to the occurrence of a fast, life-threatening arrhythmia, ventricular tachycardia (VT) or ventricular fibrillation (VF).5 However, the underlying reasons for developing these conditions are multiple (Box). In adults aged over 35 years, coronary artery disease (CAD) is the most common underlying cause of sudden death and is present in more than 80% of cases.
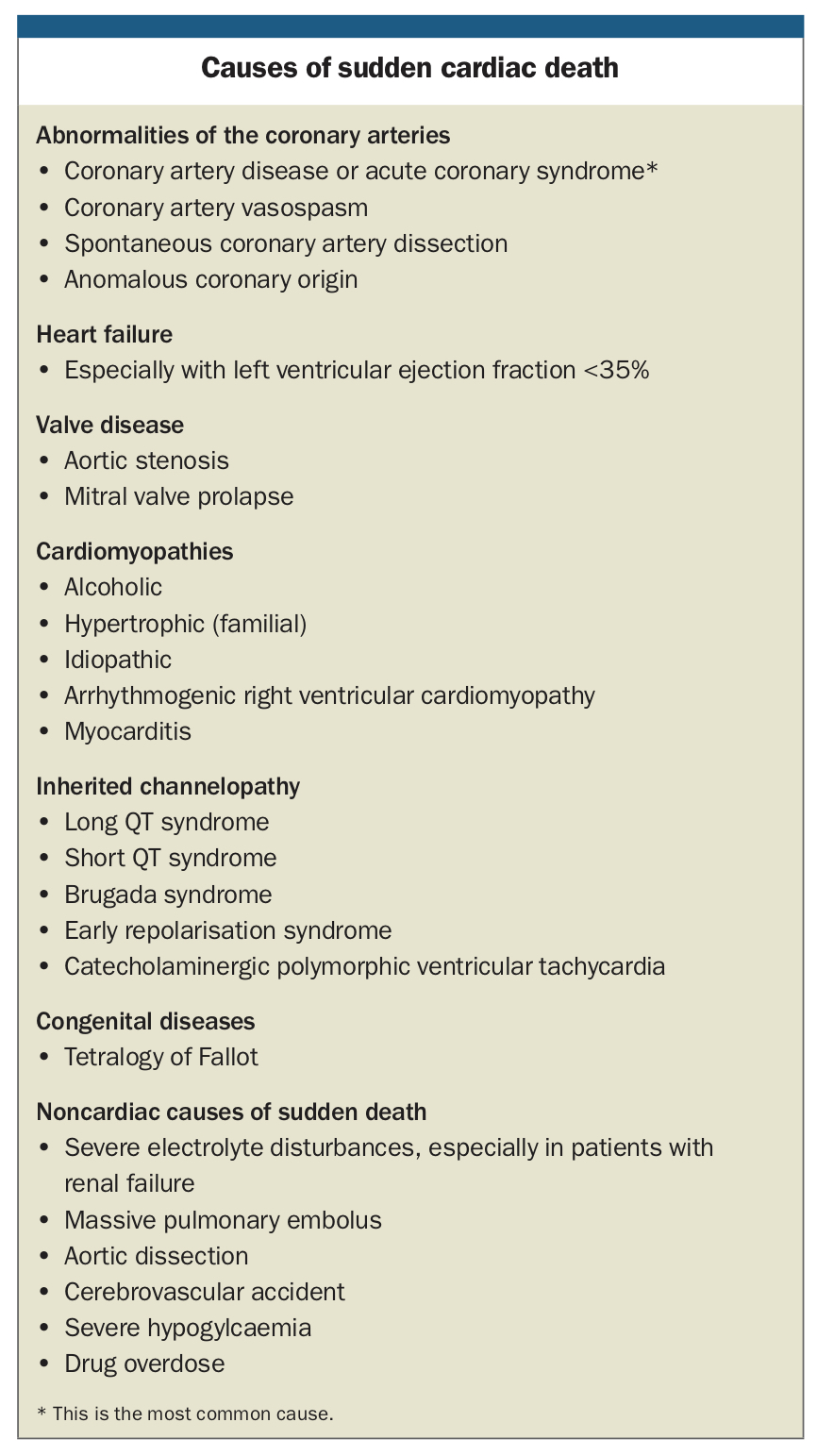{kind=link}
In the setting of coronary artery disease, sudden death can occur during an acute MI, because of electrical instability, or from old scarring of the heart. An infarction scar can result in VT or VF shortly after the MI, or even years later.
Traditional risk factors remain important predictors of SCD in the primary care setting and after an MI. These factors include older age, male sex, a personal history of hypertension, diabetes mellitus, dyslipidaemia, a family history of premature CAD or sudden death and current or past smoking. The incidence of SCD increases with age and is three to four times more common in men than in women.6 Cardiac function, as determined by the LVEF, is the most important predictor of SCD in MI survivors. Patients with a previous MI and an LVEF less than 35% are considered at highest risk.7
In young people (less than 35 years of age), genetic cardiac conditions are the more common cause of sudden death. These include inherited cardiomyopathies and primary arrhythmia syndromes.8 Specific genetic causes of SCD are further explored in the Table. These conditions are uncommon and best managed in specialised care.
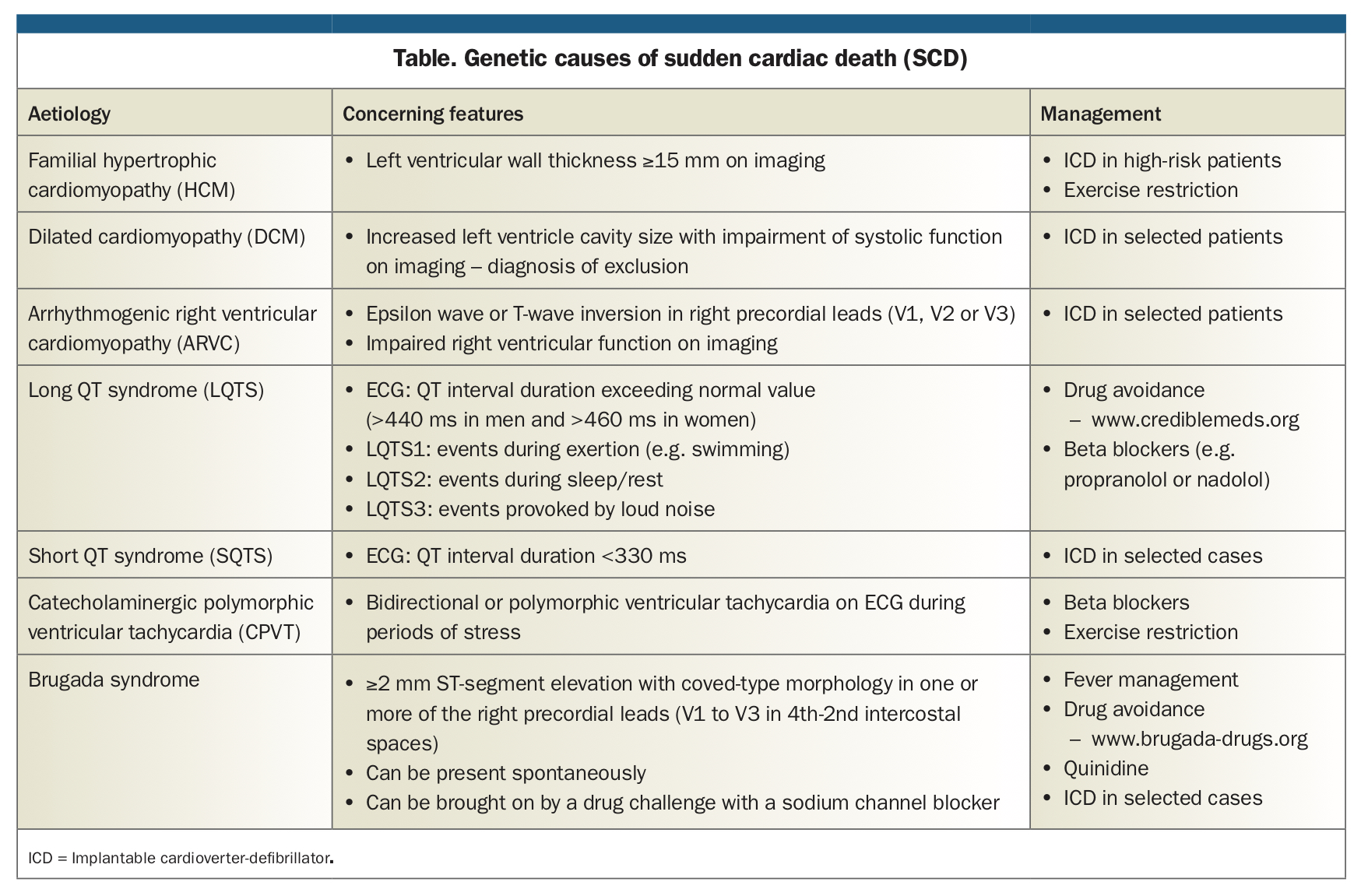{kind=link}
What tests should be performed to assess risk of SCD?
Many tests can potentially be required to assess risk of SCD or to investigate patients who have had an aborted SCD (cardiac arrest).9 A pathway for investigation and diagnostic workup in patients at risk for SCD or with suspected cardiac syncope is provided in the Flowchart.
Initial tests include an ECG to look for evidence of ischaemia, new or old myocardial infarction, left ventricular hypertrophy, an abnormal QT interval, and for the presence of a Brugada-type pattern. Some examples of ECG abnormalities that can help identify underlying cardiac disease predisposing to SCD are shown in Figures 1a to 1d.
{kind=link}
Echocardiography is also useful initially to assess for ventricular function, cardiomyopathies, enlargement of the ventricle wall and valve disease. In certain situations, a coronary angiogram, exercise stress test, electrophysiological testing, cardiac MRI and cardiac biopsy may be indicated; however, all these require specialist review. Genetic testing may also be indicated in some cases, such as in Brugada syndrome, arrhythmogenic right ventricular cardiomyopathy (ARVC), catecholaminergic polymorphic ventricular tachycardia (CPVT), and long QT syndrome. Electrophysiological studies can be performed in specific situations to aid in the diagnosis or to further stratify risk for SCD. This can include electrophysiological testing for inducible ventricular tachycardia after an MI or in patients with infiltrative cardiomyopathy. If VT can be triggered during an electrophysiological study, then the patient may be at risk for future spontaneous VT and benefit from a preventive defibrillator.
Sudden cardiac death prevention
The following preventive measures are available for people at risk of SCD:
- An implantable cardioverter-defibrillator (ICD) is a battery-powered device placed under the skin with a shock lead placed via the subclavian vein into the heart (Figure 2). If VT or VF is detected the device can briefly pace the heart faster than the ventricular rhythm or, if this is not successful in terminating it, deliver a shock. The ICD is also capable of acting as a pacemaker. Patients require specialist review and care for ICD implantation. Most current cardiac devices come with the availability of home monitoring. GPs should refer any concerning alerts, for example patients who have received therapy from the device for specialist review, as device setting or pharmacological therapy changes might be needed.
- Beta blockers should be prescribed in patients with long QT syndrome to reduce risk of sudden death.
- Underlying causes should be treated (e.g. revascularisation in coronary artery disease).
- High-risk subgroups such as athletes can be considered for screening.10
- Automatic external defibrillators in the community have been shown to improve outcomes compared with cardiopulmonary resuscitation only.
{kind=link}
Use of implantable cardioverter-defibrillators
When is an ICD appropriate?
ICDs are most commonly used in survivors of cardiac arrest or in patients who have experienced a long-lasting episode of VT. These patients would also be treated with beta blockers and occasionally other antiarrhythmic therapy such as amiodarone. ICDs may also be used for primary prevention of SCD in those with low LVEF (<30 to 35%) after an MI and in some patients with hypertrophic cardiomyopathy.3
In patients with ischaemic heart disease, a preventive ICD should be considered 40 to 90 days after a myocardial infarction. Indications are:
- LVEF ≤35% with heart failure symptoms
- LVEF ≤30% without heart failure symptoms.
In patients with nonischaemic cardiomyopathy, a preventive ICD should be considered when:
- LVEF ≤35%, despite appropriate anti-heart failure medications. However, a recent trial has shown that there might not be a similar benefit in patients with cardiomyopathy who do not have coronary artery disease.11
- they have had a cardiac arrest or documented sustained VT or VF not due to a reversible cause.
Driving and ICDs
Patients with an ICD have specific licensing conditions for driving. Information about the special conditions can be accessed on the Austroads website (https://austroads.com.au).12 In general, patients with an ICD can hold a private vehicle licence after meeting set criteria (i.e. no driving for six months after a cardiac arrest); however, patients with an ICD cannot hold a commercial vehicle licence.
Alternative devices
There are newer alternatives to implantable defibrillators. These include a wearable cardiac defibrillator (often called a vest) and a subcutaneous defibrillator. Wearable defibrillators are often considered in patients with a reversible risk of SCD. Subcutaneous defibrillators can be considered in patients in whom leads within the heart would not be clinically suitable, such as the presence of ongoing bacteraemia.
Palliation and ICDs
Management of patients with a pre-existing ICD who are approaching the end of life is often undertaken by the treating GP. It is usually not appropriate for ICDs to remain active and deliver shocks to the heart. Deactivating an ICD may allow patients to have a peaceful death. About 20% of ICD patients receive shocks in the last weeks, days or hours of their lives. The decision to deactivate an ICD can be made by the patient’s treating physician in consultation with the patient, their family and the patient’s cardiologist. Cardiac devices need to be removed before cremation because of potential damage to the crematory chamber from flying metal, but a patient may be buried with their device in situ.13
When to refer for specialist care
Patients with concerning symptoms or a history suggestive of an increased risk for SCD should be referred for review by a cardiologist. Any patient with concerning symptoms, who is under 35 years of age and/or has a family history of SCD or unexplained cause of death should be considered for referral to a specialist genetics clinic for further investigation.
When should you not complete a death certificate?
The coronial legislation in each state and territory varies. However, in general, a death should be reported to the Coroner if the cause of death is unknown, or if the person was not attended by a medical practitioner within a certain period before death, for example, three months in the ACT or six months in NSW. Reporting all potential sudden deaths to the Coroner is vital, as an autopsy in this situation can help with risk stratification for the family.14
Conclusion
SCD has devastating consequences for families. Early recognition of patients at risk of SCD and awareness of genetic causes for SCD has an important impact on not only the affected person but also their family members. The GP is at the forefront with regard to SCD in the community and is an integral member of the multidisciplinary team caring for families affected by SCD and survivors of cardiac arrest. CT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.