‘I have a narrowing in my heart artery and they don’t need to fix it?’ Impact of the ISCHEMIA trial

Coronary artery disease
The literature on invasive versus noninvasive treatments for stable angina has amassed, with significant implications for GPs and specialists alike. Both types of therapy have shown a reduction in morbidity associated with stable coronary artery disease; however, patient-tailored treatments should be guided by recent clinical trial evidence.
- There are a variety of treatment options for patients with stable angina, including invasive and noninvasive strategies.
- Medical therapy targeting cardiovascular risk factors is the cornerstone of treatment of patients with coronary artery disease, and the GP has a central role in risk factor management.
- Medical therapy should be optimised irrespective of whether an additional invasive approach is used.
- Pharmacological therapy can be effective in controlling symptoms of stable angina.
- In patients who have ongoing angina despite maximally tolerated pharmacological therapy, percutaneous coronary intervention (PCI) has an important role in relieving symptoms and potentially improving quality of life.
- PCI is not offered for prognostic benefit in patients with stable angina.
Case scenario
A 67-year-old man has returned for follow up in your general practice after consulting a cardiologist for weekly episodes of chest pain. He has a background history of hypertension, prior smoking and sedentary lifestyle. The cardiologist performed a stress test and the results were abnormal. The patient subsequently underwent a coronary angiogram and was told he had a 70% blockage in his right coronary artery. It was recommended that he be treated with risk factor modification and medical therapy. The patient expresses bewilderment that the 70% narrowing was not stented.
In Australia, coronary artery disease (CAD) remains the leading cause of death.1 The common clinical presentations of CAD include angina (stable or unstable), myocardial infarction, arrhythmia and heart failure. Stable angina is caused by a fixed coronary stenosis, leading to a supply/demand imbalance of blood flow with exertion or stress, resulting in myocardial ischaemia. It is important to apply evidence-based management to patients with this common problem. Options for management include invasive approaches or medical approaches, often termed medical therapy (MT). The early invasive approach to acute coronary syndromes (ACS) has been shown to improve cardiovascular outcomes.2 In this review, we discuss the current gold standard approach to the management of stable angina in light of the evidence from randomised clinical trials.
Invasive therapy
Invasive methods of treating significant coronary artery lesions are either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG). The choice of treatment depends on anatomical features, patient comorbidities and patient preference. Contemporary PCI applies use of drug-eluting stents, which elute antiproliferative medications into the endothelium to prevent re-stenosis. Furthermore, detailed haemodynamic assessments and intravascular imaging enable accurate lesion characterisation and intervention and have become the standard of care for contemporary PCI.3 The procedure is performed under sedation, using local anaesthetic, and can usually be performed through a small sheath in the radial artery. Same-day discharge is feasible for most patients undergoing PCI. Contemporary CABG applies maximal use of arterial grafts, improving graft longevity.4 There are options for minimally invasive direct coronary artery bypass (MIDCAB) through minithoracotomy, which is occasionally offered for suitable patients.
Medical therapy
MT includes cardioprotective therapy such as:5,6
- antiplatelet therapy (which reduces major adverse cardiovascular events [MACE] in patients with known CAD; however, this benefit is mostly seen in patients with ACS)7
- a beta-1 selective antagonist titrated to the maximally tolerated dose
- an ACE inhibitor such as ramipril or perindopril, as there is evidence that these ACE inhibitors have a MACE benefit7
- lipid-lowering therapy, usually in the form of statins8
- lifestyle-related measures including smoking cessation, weight loss, exercise for more than 150 minutes per week
- measures for controlling diabetes.
In addition to the cardioprotective therapy outlined, antianginal therapy can be used to improve symptoms.9 These medications have varying degrees of antianginal potency and differing side-effect profiles.
First-line antianginal therapy would include beta-selective antagonist therapy. If this is ineffective, nitrates and nicorandil may be trialled, which improve ischaemic symptoms through vasodilatory mechanisms. Tolerance of these drugs may be limited by the effect on blood pressure. Nondihydropyridine calcium antagonists such as verapamil and diltiazem reduce myocardial oxygen demand through chronotropic effects and may be effective in controlling angina; however, these drugs should be avoided in patients with heart failure. Perhexiline works by modulating mitochondrial metabolism from fatty acid to glucose utilisation, resulting in increased adenosine triphosphate production for the same oxygen consumption, and consequently increases myocardial efficiency. Perhexiline may be offered in cases of refractory angina. It is not commonly used due to a significant adverse-effect profile, including neuropathy and hepatitis.
What does the evidence say?
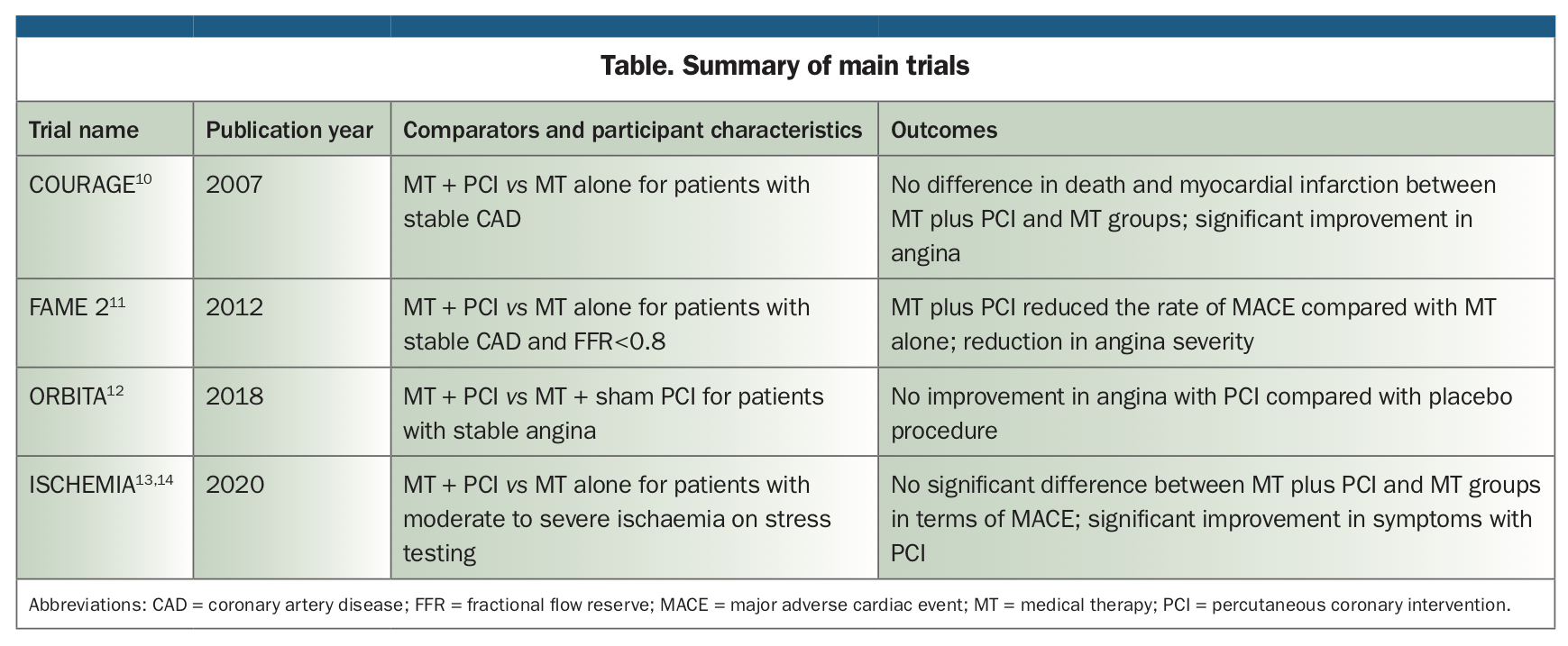
Several landmark studies have aimed to answer the question of whether PCI or MT is most appropriate for patients with stable angina. These include the COURAGE (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation), FAME 2 (Fractional Flow Reserve-Guided Percutaneous Coronary Intervention Plus Optimal Medical Treatment Versus Optimal Medical Treatment Alone in Patients with Stable Coronary Artery Disease), ORBITA (Objective Randomised Blinded Investigation With Optimal Medical Therapy of Angioplasty in Stable Angina) and, most recently, ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trials (Table).10-14
{kind=link}
The COURAGE trial of 2007 compared cardiovascular events for patients with stable coronary disease treated with MT with or without PCI.10 This study found no difference between PCI and MT in terms of its primary endpoint of MACE, a composite of myocardial infarction, stroke, heart failure, recurrent revascularisation and cardiovascular death. However, COURAGE identified a significant improvement in angina severity with PCI compared with MT. The conclusions from this trial were confounded, as one-third of patients randomised to MT ended up receiving PCI, and PCI was performed with bare metal stents, a technology that is largely redundant in the current era.
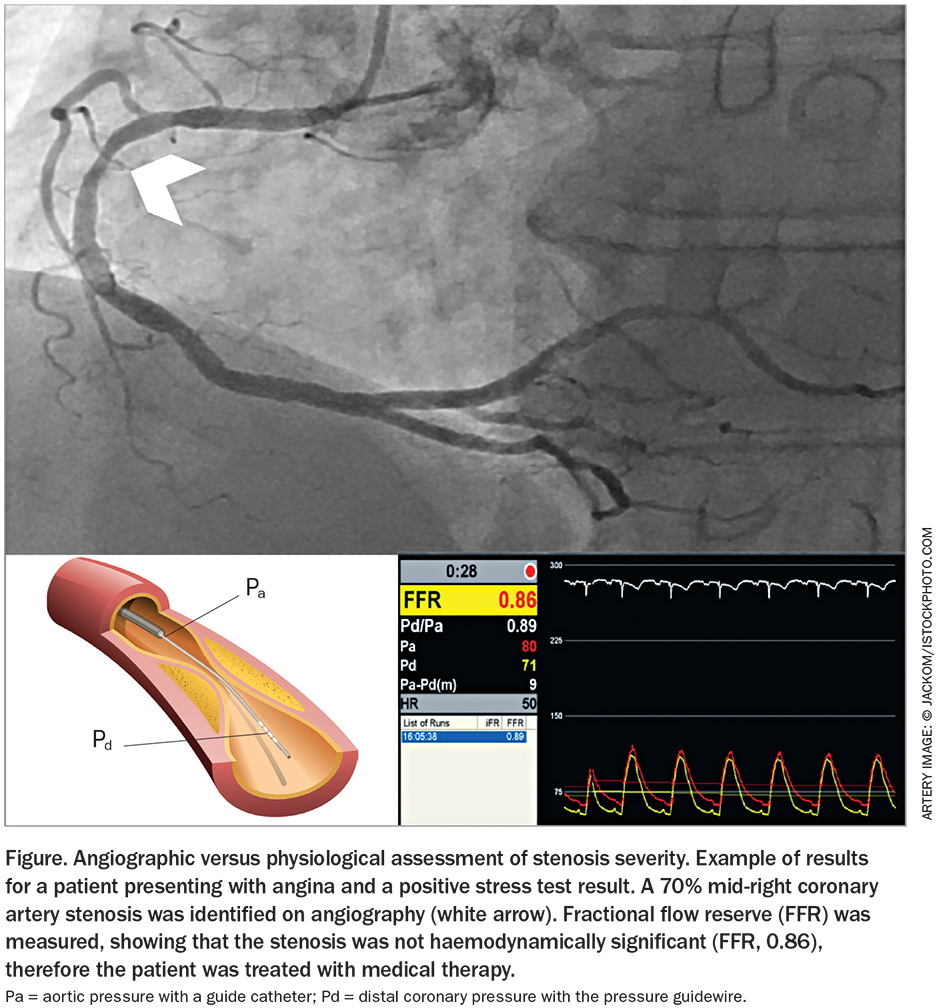
Since this trial, there have also been developments in the physiological assessment of lesion severity through pressure wire assessment, which has enabled targeted use of PCI for haemodynamically significant lesions. Physiological assessment of lesion severity involves measuring maximum blood flow distal to a stenotic lesion (Pd) compared with normal maximum flow proximal to the lesion (Pa) through a specialised pressure wire, generating a ratio (Pd/Pa). The technologies in routine use for physiological assessment include fractional flow reserve (FFR), which involves medication administration to maximise flow through a lesion, and instantaneous wave-free ratio (iFR), which calculates the Pd/Pa in a period of diastole of least microvascular resistance (the wave-free period), thereby allowing measurement of maximum flow without medication administration (Figure). The rationale for these technologies is to identify significant lesions that restrict blood flow, rather than relying on anatomical grading of severity alone.
{kind=link}
In the landmark FAME 2 trial, patients with stable CAD and a physiologically significant lesion (FFR of ≤0.80) were randomised to either MT plus PCI or MT alone.11 In contrast to the COURAGE trial, FAME 2 showed a significant reduction in MACE (primarily driven by need for urgent revascularisation) in patients receiving PCI compared with those receiving MT, and confirmed the findings of COURAGE, with a reduction in angina severity in patients randomised to physiologically guided PCI compared with those receiving MT. This advantage of physiologically guided PCI over angiography alone appears to be a ‘class effect’, with both the DEFINE-FLAIR and iFR-SWEDEHEART studies demonstrating the reliability of iFR as a valid alternative to FFR, with iFR ≤ 0.89 considered significant.15,16 As a result of these trials, both modalities have become common in clinical practice and are mandated in international guidelines to guide revascularisation in the absence of other tests demonstrating objective ischaemia.17,18
More recent trials have, however, further nuanced the management of stable angina. In the ORBITA trial, patients with stable angina and single vessel CAD already receiving MT were randomised to either PCI or a sham procedure to assess for angina improvement.12 This study found that PCI did not provide any additional improvement in angina, as measured by treadmill exercise time, compared with the sham procedure. This was despite the fact that most lesions were haemodynamically significant, with a mean FFR of 0.69 and mean iFR of 0.76. However, 30% of patients did not have a haemodynamically significant lesion, and therefore PCI in this subgroup possibly diluted the benefit that may have been seen if the study were limited to only haemodynamically significant lesions based on physiological assessment.
The ISCHEMIA trial was designed to be the final say on the optimal management of stable angina, with 5179 patients with proven moderate to severe ischaemia on stress testing randomised to either MT plus PCI or MT alone.13,14 At 5 years, there was no significant difference for the primary endpoint of MACE between the two groups. However, as was seen in the earlier studies, patients who underwent PCI derived significantly greater improvement in angina compared with those receiving MT alone, and this was most pronounced in patients with more frequent angina at baseline.14 It should be further noted that of the patients randomised to the MT group, 26% underwent angiography, and 21% of this subgroup underwent PCI as a result of failure of MT, which again may confound the interpretation of results. Furthermore, the findings of this trial do not apply to patients with significant left main CAD (>50%), low ejection fraction, moderate to severe heart failure symptoms (New York Heart Association class III or IV), or those who are very symptomatic despite the use of MT at maximum acceptable doses, as such patients were excluded from the trial.
Patients with renal impairment were further examined in the ISCHEMIA CKD trial, in which patients with advanced kidney disease and moderate to severe ischaemia on stress testing were randomised to MT plus PCI or MT alone.19 It was again found that overall there was no significant difference in MACE between the two groups after a median of 2.2 years of follow up. However, there was a heterogeneity depending on the extent of ischaemia, with reduced events in patients with severe ischaemia who underwent PCI as opposed to MT alone.
Conclusion
The treatment options for stable angina include invasive and noninvasive measures. The evidence indicates that MT is the standard of care for all patients. All the major trials (except ORBITA) suggest that PCI offers additional benefit to MT in improving symptoms and quality of life, and are considered class I evidence in the latest European Society of Cardiology/European Association for Cardio-Thoracic Surgery revascularisation guidelines.20
A patient such as the man in our case scenario, with a 70% right coronary artery lesion, should be counselled so he or she understands that evidence supports safe deferral of PCI and commencement of MT. Management of hypertension and lifestyle factors should be optimised to limit atherosclerotic progression. Antianginal therapy should be commenced. If symptoms are ongoing despite maximally tolerated MT, PCI should be offered to provide symptomatic benefit.
The treatment approach should always be tailored to the individual, and open dialogue between the GP, patient and cardiologist will result in the best outcomes for the patient. Early cardiologist involvement is important to define the severity of coronary disease and to treat the negative sequelae that may be associated with this. The GP is ideally positioned to target aggressive risk factor control, which is of crucial importance to limit the progression of disease and requires constant surveillance and continuity of care in order to provide the best outcomes. CT