Blood pressure management during COVID-19. Tricks and traps of home monitoring

Hypertension
The COVID-19 pandemic has led to an increase in patients performing home blood pressure monitoring (HBPM). It is important that patients have the correct equipment when performing HBPM and for GPs to provide adequate education, training and follow up to successfully manage patient health, as well as identify any comorbidities.
- The rapid transformation of healthcare provision during the COVID-19 pandemic in Australia has necessitated increased home blood pressure monitoring (HBPM).
- HBPM is an effective and reproducible method for the diagnosis and management of hypertension if performed using a standardised, evidence-based protocol.
- The COVID-19 pandemic has provided opportunities to innovate and collaborate with patients, using technology to improve health awareness, engagement and empowerment, enabling patients to perform HBPM.
- Clinicians are required to provide education and support to ensure optimal technique and response to blood pressure measurements.
The Coronavirus-19 (COVID-19) pandemic has caused widespread changes to health care provision of chronic and noncommunicable diseases. The shift from face-to-face to virtual care to minimise exposure of patients and health professionals to COVID-19 has led to increased use of self-test kits and devices to support the transition of a traditional healthcare models to home-based management. One such example is home blood pressure monitoring (HBPM), which is a validated and reliable method for diagnosis and management of hypertension. At present, there are many challenges for clinicians to provide optimal care for patients; however, hypertension remains critically important, being highly prevalent and the most common preventable risk factor for major cardiovascular events. The case study below illustrates the common tricks and traps in the management of hypertension using HBPM during the COVID-19 pandemic.
What is home blood pressure monitoring?
HBPM refers to the self-measurement and recording of blood pressure (BP) using a validated automatic device at home over several days. This is distinct from ambulatory blood pressure monitoring, where an electronic device measures and records BP every 15 to 30 minutes during the day and 15 to 60 minutes during sleep time over 24 to 48 hours. HBPM is normally indicated for patients who have high cardiovascular risk, those receiving antihypertensive treatment (approximately four weeks after any change in medications) and patients in whom the diagnosis of hypertension is clinically suspected but may be complicated by patient anxiety at clinical attendances.
Case study
A 58-year-old male smoker with a background history of hypercholesterolaemia and type 2 diabetes was diagnosed with hypertension six months ago by his GP on the basis of persistently elevated BP readings (165/106 mmHg) on two separate visits. Clinical examination revealed an elevated body mass index of 33.5 kg/m2 (moderate obesity) and microalbuminuria (albumin:creatinine ratio 1 mg/mmol, >2.5 mg/mmol is abnormal) with no evidence of hypertensive retinopathy on fundoscopy. He was commenced on perindopril 5 mg once daily but this failed to achieve adequate BP control. Amlodipine was subsequently added and both agents were titrated to ceiling doses. He returned for follow up via telehealth consultation. His home BP readings, measured using a wrist band device, showed an average day-time BP of 150/95 mmHg despite stating compliance with his medications.
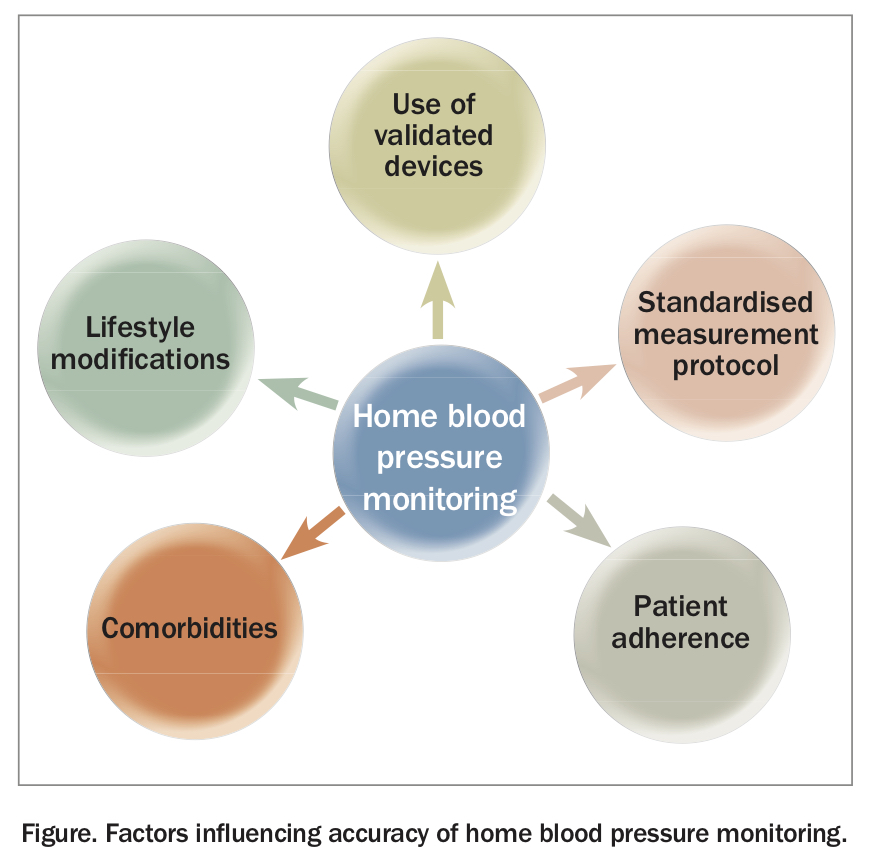
Several factors can influence the reliability of home BP readings and these include the proper selection of equipment, the technique and timing of measurements as well as patient factors (Figure). It is therefore crucial to evaluate these factors at each visit to assure a truly accurate reading before any modifications of antihypertensive medications.
{kind=link}
Equipment and technology
Accurate HBPM requires the correct equipment. A list of upper arm devices for self-measurement of BP that have been validated by the British Hypertension Society and the European Society of Hypertension is available at www.dableducational.org/index.html. Both wrist and finger cuff monitors should be avoided as they are extremely sensitive to body position and less likely to have passed validation testing. Inappropriate cuff size has also been associated with inaccurate recording of BP results; a cuff size that is too small results in overestimation of BP while a cuff size that is too large results in underestimation. The cuff bladder should encircle at least 80% of the arm circumference of the adult user.1 This may be an issue in obese patients, where an extra-large cuff (frequently referred to as a thigh cuff) may be required to obtain an accurate brachial measurement of BP. If a suitable cuff cannot be obtained, then wrist BP measurement, with the wrist held at the level of the heart, is the best alternative option.2
Training, education and technique
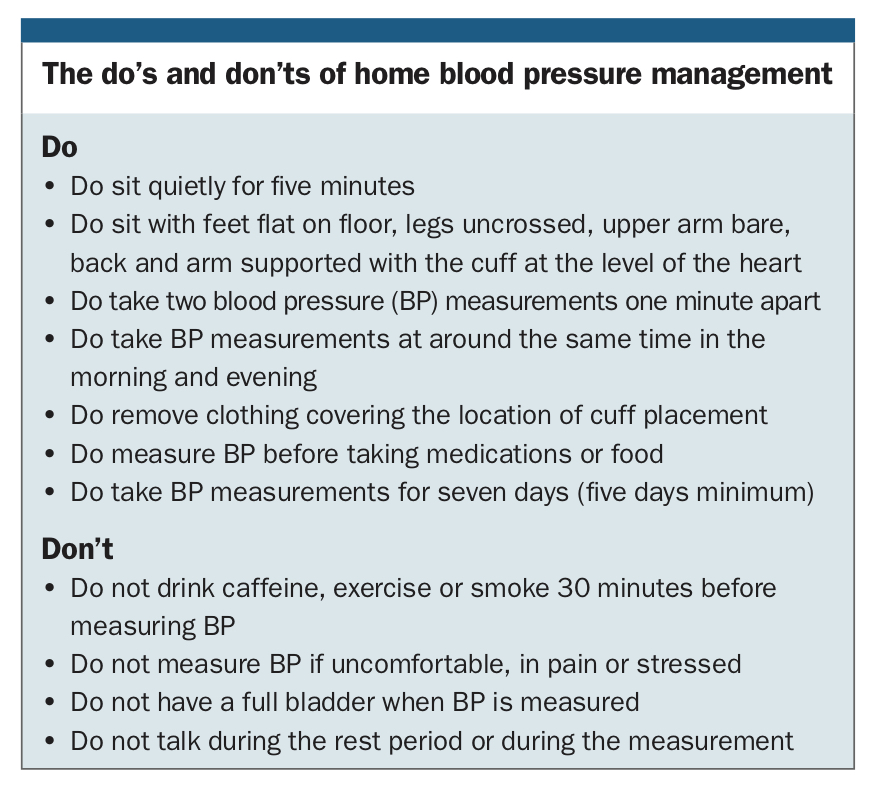
Patients are required to rest for five minutes before BP measurement is taken. Repeated studies have shown that few participants followed all of the recommendations for HBPM, including ‘5 minutes rest, no talking, legs not crossed, back supported, quiet setting’.3 Lack of adherence to these recommendations highlights the importance of providing detailed education and support for patients on the optimal technique for measuring their own BP to minimise error. Additionally, patients benefit from having the BP cuff size and fit reviewed and their technique witnessed and corrected before starting HBPM. A list of the ‘dos and don’ts’ of HBPM is summarised in the Box.4 Detailed written education supports are available for patients and clinicians at www.heartfoundation.org.au/getmedia/aaa139aa-d586-4b93-8d2a-8f857f0cd2eb/Measuring-your-blood-pressure-at-home.PDF.
Elderly individuals in whom arterial stiffening is prevalent or in people with autonomic neuropathy such as those with diabetes can experience orthostatic hypotension that could potentially lead to syncope and falls. Therefore, it is helpful to advise these patients to measure BP in duplicate while seated and immediately when standing to assess for postural hypotension.
Patient adherence
Nonadherence to diet and medications is one of the main contributing factors of suboptimal BP control and it is an indicator of poor prognosis in hypertensive patients. Adherence to antihypertensive therapy should be evaluated as appropriate at each visit (or telehealth consultation) and before escalation of treatment. Strategies to improve medication adherence include:
- use of single pill combinations
- once-daily dosing medications
- use of medication reminder packaging
- empowerment-based counselling for self-management
- provision of regular feedback to patients.5
HBPM in conjunction with hypertension education has the potential to improve health literacy for hypertensive patients, which is an essential component in the long-term management of hypertension.
Case study continued
The patient bought a validated upper-arm BP monitor and, after adopting the standardised protocol for HBPM, returned for a second telehealth consultation with his BP diary. He took both antihypertensive medications in the morning and reported an average premedication morning BP of 149/90 mmHg and an evening BP of 124/75 mmHg. He had normal kidney function, an elevated total cholesterol level of 6.0 mmol/L (HDL cholesterol, 1.8 mmol/L and LDL cholesterol, 3.7 mmol/L) and glycated haemoglobin level of 6.7%.
He was feeling a little tired during the day and had stopped going to gym during the COVID-19 pandemic. He had also become nonadherent with a low salt diet and was drinking a little more alcohol than one standard drink a day. Given the possibility of antihypertensive medications contributing to lethargy and morning BP surge, he was advised to switch to night-time dosing, and nonpharmacological interventions were also discussed in detail. He also was referred to a dietitian who does telehealth consults and plans to reattend the gym when COVID-19 restrictions allow.
The benefits of HBPM
Over the past two decades there has been increasing evidence that HBPM is useful and accurate in diagnosing and monitoring hypertension, if it is performed according to a recommended protocol (Box). The criteria for the diagnosis of hypertension based on HBPM is an average reading over at least three days of systolic blood pressure ≥135 mmHg or diastolic blood pressure ≥85 mmHg.6 Compared with clinic assessment of BP, HBPM provides additional advantages including:
{kind=link}
- detecting masked hypertension, where BP is within normal limits in clinic and elevated at home
- detecting white coat hypertension, where BP is elevated in clinic but normal at home.
In addition, HBPM can be used to capture day-to-day BP variability and clinical response after adjustment of antihypertensive regimens. Patients are encouraged to record BP measurements to aid in assessment at consultation. An example of the HBPM diary can be downloaded at https://www.racgp.org.au/download/Documents/AFP/2016/January/February/
Fig2_Home_BP_diary.pdf.
The significance of a morning blood pressure
It is well established that nocturnal hypertension (also known as nondipping, where BP does not drop by 10%), recorded by ambulatory blood pressure monitoring, is a strong independent predictor of sudden cardiovascular events in patients who are hypertensive. When added to the morning surge phenomenon, which refers to early morning BP ≥135/85 mmHg at home immediately on waking and before taking morning tablets, it signifies very high long-term cardiovascular risk in patients. However, the optimal timing for antihypertensive medication administration remains a controversial topic on a background of highly debated results from several major clinical trials. Notwithstanding, night-time antihypertensive dosing may help to improve adherence by minimising common side effects such as lethargy from certain antihypertensive classes.
Lifestyle modification
In addition to pharmacological treatment, lifestyle measures can reduce cardiovascular risk and enhance the effects of antihypertensive treatment. The estimated Framingham 10-year risk of cardiovascular disease for the patient in the case study was 53.5%, which makes cardiovascular risk-factor control a key priority. Lifestyle modifications such as reducing salt intake (<5 g/day), dietary modification (including a diet rich in whole grains, fruits, vegetables, polyunsaturated fat and dairy products), moderation of alcohol intake, weight reduction, smoking cessation and regular physical activity should be addressed and emphasised. Excessive caffeine or energy-drink consumption should be avoided. Moreover, the implication of the pandemic on mental health should not be overlooked as chronic stress and depression have also been associated with hypertension.7 Patients should therefore be encouraged to adopt strategies to help reduce stress including introducing mindfulness or meditation into their daily routine, getting adequate sleep and exercise, and strengthening social networks and supports.
Management of comorbidities
In addition to cholesterol management, evaluation for obstructive sleep apnoea should be considered in overweight individuals where clinical history is suggestive (e.g. daytime somnolence, snoring, witnessed episode of apnoea during sleep) as this may identify an important contributing factor to hypertension that may require treatment with continuous positive airway pressure support or surgery to correct anatomical obstruction.
Conclusion
Although the increase in virtual or physically distant care has been driven by the need to reduce the exposure to people with COVID-19, this pandemic could be seen as an impetus for sustainable change in hypertension management by delivering effective HBPM with a supportive model of care based on collaborative partnerships between GPs, specialists, nurses and pharmacists. Patients’ preferences for care and access are variable and continue to evolve over time and therefore healthcare systems must constantly adapt to improve care to meet patients’ expectations and needs. CT
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.