Lipid management – what counts, what is new?
Professor Simons is Associate Professor of Medicine at UNSW Sydney and the Lipid Research Department, St Vincent’s Hospital, Sydney, NSW.
Lipid disorders
Heart diseases--prevention
People with elevated lipid levels are at increased risk of developing cardiovascular disease. Lipid-lowering therapies including statins, ezetimibe and PCSK9 inhibitors have been shown to mitigate these risks. A number of new therapies are in the pipeline that show efficacy in lipid management.
- Lipid-modifying therapy will reduce cardiovascular disease (CVD) risk in many patients, especially in those with pre-existing CVD.
- There remains a large unmet need for better CVD prevention via lipid control.
- Many patients are not receiving lipid therapy according to guidelines.
- In addition to statins and ezetimibe, PCSK9 inhibitors offer additional CVD prevention.
- There are several new drugs in development that will assist in lipid management.
- The guidance underlying lipid management is clear – intensive lipid therapy is required in secondary prevention and less intensive therapy, applied selectively, is required in primary prevention.
Blood lipid abnormalities, especially raised levels of low-density lipoprotein cholesterol (LDL-C), are causally related to atherosclerotic cardiovascular disease (CVD). Elevated levels of triglyceride-rich lipoproteins (often simply expressed as elevated triglycerides) and lipoprotein(a) are also associated with increased risk of CVD, as are low levels of high-density lipoproteins (HDL). The purpose of this article is not to revisit the epidemiology of CVD, rather, it is to consider what lipid therapy can achieve now and what progress lies ahead.
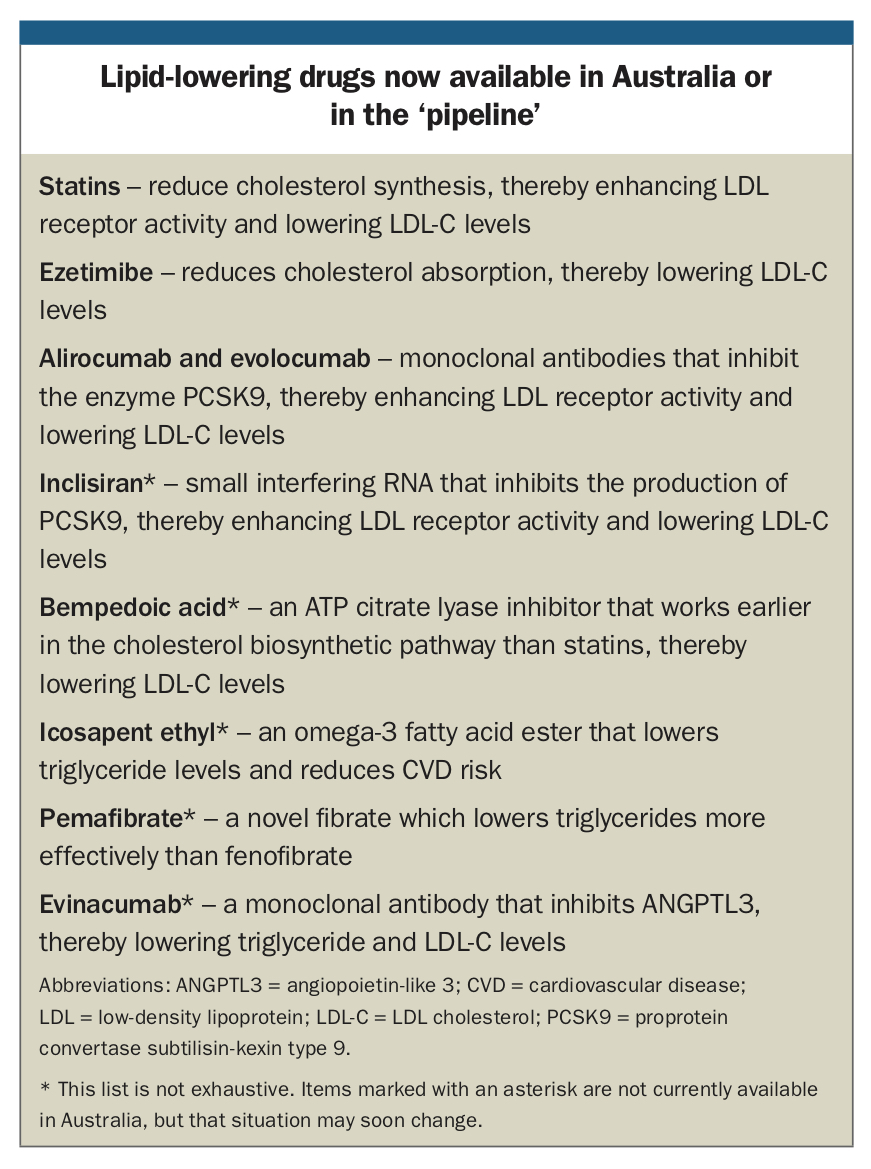
Although there have been a number of lipid-modifying drugs available since the 1960s, over the past 30 years we have witnessed the development of many new lipid-lowering therapies. Lipid-lowering therapies available in Australia and those in development are outlined in the Box.
{kind=link}
What does lipid-lowering therapy achieve beyond observed changes in lipid profile?
Various lipid-lowering interventions have been clearly shown to reduce CVD risk. The evidence is strongest for statin drugs, but also exists for ezetimibe and proprotein convertase subtilisin-kexin type 9 (PCSK9) inhibitors.1-4
Randomised trials demonstrate that statin therapy reduces the relative risk of a major CVD event by about 25% for each 1 mmol/L reduction in LDL-C during each year after the first year that it continues to be used.1 That is to say, there is a lag time before onset of CVD benefit.
In simple patient parlance, statin therapy in 10,000 patients for five years would prevent:
- about 1000 CVD events in those with pre-existing CVD (secondary prevention)
- about 500 CVD events in those with elevated CVD risk but no pre-existing CVD (primary prevention).
Considerable residual CVD risk in patients remains despite conventional lipid-lowering and other therapies. This residual risk might be attributed, at least in part, to a continuing excess of LDL-C and other lipoproteins, and to other risk factors, known or unknown. In addition, a small proportion of patients are unable to tolerate a full or any dose of statin. 5
Lipid management guidelines mandate that patients undergoing secondary prevention should receive intensive statin therapy, usually meaning high-dose atorvastatin or rosuvastatin (with or without the addition of ezetimibe).6,7 An Australian study of 3441 patients who were acute coronary syndrome survivors (i.e. essentially heart attack survivors), found that only 55% were receiving intensive lipid-lowering therapy at six or 12 months follow up and 22% were receiving no lipid-lowering therapy at all.8 Potential reasons underlying this ‘treatment gap’ are complex, but are both medical and sociological. However, it is unlikely that 45% of heart attack survivors on intensive statin therapy suffered side effects so severe as to dictate a change in therapy.5
What is the role of PCSK9 inhibitors?
Administration of PCSK9 inhibitors leads to reduction in LDL-C level of around 50% and this is additive to the effect of any concurrent statin therapy.9 This therapy may also reduce lipoprotein(a) by 25 to 30%, which may ultimately be an important outcome.10,11
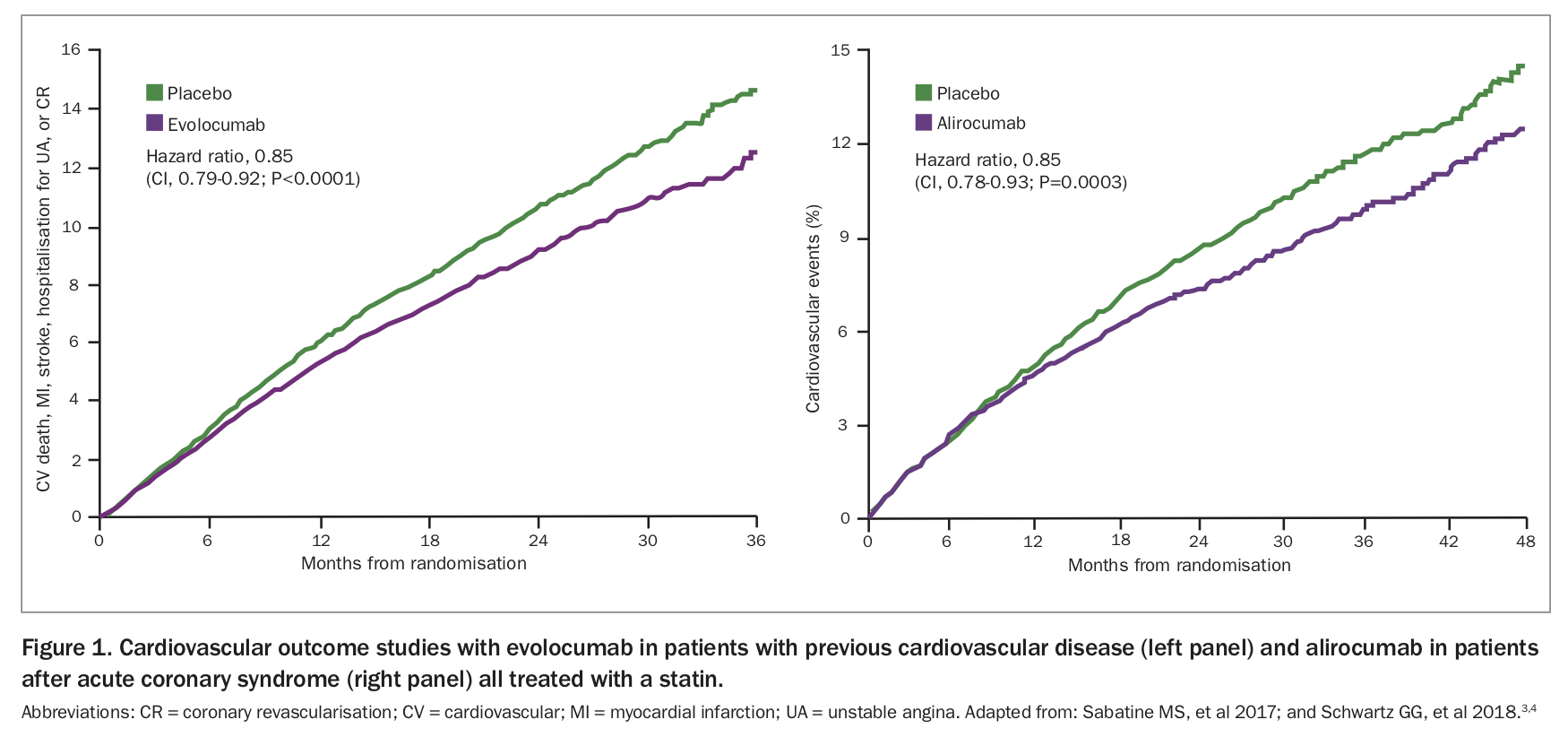
In large secondary prevention trials involving patients concurrently receiving statins, both evolocumab and alirocumab significantly reduced the relative risk of a first CVD event by an additional 15% compared with placebo injections (Figure 1).3,4 Furthermore, the total number of nonfatal CVD events and deaths prevented was twice the number of ‘first events’ prevented.12 Treatment with either inhibitor was well tolerated and adverse event rates were similar to placebo, except for a slight excess of injection-site reactions.3,4
{kind=link}
No similar clinical trial data are available in the context of primary CVD prevention. However, the use of PCSK9 inhibitors is encouraged in patients who are at high CVD risk but have no pre-existing CVD, but this is on an empirical basis.7
PCSK9 inhibitors are self-injected subcutaneously at intervals of two or four weeks. The maximum reduction in LDL-C level is achieved when a PCSK9 inhibitor is used in combination with statin and/or ezetimibe.9 Largely because of high cost, alirocumab or evolocumab will generally be used as a supplement to conventional treatment in patients needing further help to reach LDL-C target levels. They may also be used as solo therapy (or combined with ezetimibe) in patients intolerant to statins.
PCSK9 inhibitors are PBS-subsidised in Australia for patients with familial heterozygous hypercholesterolaemia or for those with nonfamilial hypercholesterolaemia who are at high cardiovascular risk. PBS subsidy guidelines for PCSK9 inhibitors are complex and practitioners are advised to consult detailed PBS information.13
New drugs: inclisiran and bempedoic acid
PCSK9 synthesis and activity may also be reduced by a small interfering RNA known as inclisiran. This drug is given by subcutaneous injection, effectively reduces LDL-C levels by at least 50% and may only need administration once every six months.14 The results of CVD outcome studies are awaited.
Bempedoic acid is an orally administered product that works earlier in the cholesterol biosynthetic pathway than statins.15 It is a prodrug, not activated until reaching the liver. Hence, it is not active in muscle and potential muscle adverse effects associated with statins may be avoided.16 It has been shown to reduce LDL-C levels by at least 20%.15 Subject to favourable CVD outcome studies and safety considerations, this drug may represent an important future option in lipid-lowering therapy.
Triglyceride-lowering drugs
After comorbid conditions such as diabetes, obesity, hypothyroidism or ‘sensitivity’ to alcohol or certain drugs have been addressed, the remaining options in triglyceride management are fibrates or omega-3 fatty acids.17
Fenofibrate has been shown to reduce CVD risk in type 2 diabetes, but only when triglyceride levels are above 2.0 mmol/L and HDL level is below 0.9 mmol/L.18,19 Pemafibrate is a novel fibrate with higher potency than fenofibrate and more selectivity for the PPARα receptor.20 Pemafibrate may reduce triglyceride levels by around 50% and there are few drug-drug interactions, even with statins.20 The results of a CVD outcome study in type 2 diabetes in patients with elevated triglycerides and low HDL level are awaited.
Omega-3 fatty acid supplementation (using supplements usually derived from marine sources) has long been known to reduce elevated triglyceride levels in responsive patients. However, reviews and meta-analyses have not confirmed significant CVD prevention.21,22 A recent study administered either high-dose, pure eicosapentaenoic acid ester (icosapent ethyl) or placebo to 8179 patients with established CVD or diabetes who had elevated triglyceride levels and were concurrently using statins.23 Triglyceride reduction was 20% greater and absolute CVD event reduction 4.8% greater in patients on icosapent ethyl, yielding a favourable number needed to treat to prevent one event of only 21.23 The mechanism underlying this significant CVD prevention is uncertain, but this product may become available in Australia in the near future.
Evinacumab, a monoclonal antibody that inhibits the triglyceride metabolism regulator angiopoietin-like 3 (ANGPTL3), has been shown to reduce triglyceride levels by 70 to 80% in patients with hypertriglyceridaemia and to reduce LDL-C levels by at least 50% in patients with refractory hypercholesterolaemia.24,25 This product may have a future role in CVD prevention.
Lipid management guidance
Intensive lipid-lowering therapy is essential in most instances of secondary CVD prevention.6,7 Less intensive therapy is indicated in primary prevention, but with some consideration of the overall clinical picture. Such considerations include severity of the lipid problem, the presence of other CVD risk factors, perhaps the results of a coronary artery calcium score, comorbidity, and demographic and other personal factors. Lipid therapy will generally be permanent in nature, once a patient has been stabilised.
In secondary prevention, an LDL-C target level is still notionally 1.8 mmol/L in Australia, but many authorities are suggesting the need for a lower target.17 In primary prevention the target is 2.0 mmol/L or lower. A target non-HDL level of 2.5 mmol/L is also suggested, as this does not require fasting and takes into account the cholesterol content of triglyceride-rich lipoproteins and remnants.
In hospitalised patients with acute coronary syndrome, lipid therapy will be high-dose atorvastatin or rosuvastatin according to protocol. In general practice, patients with an elevated LDL-C level may be started on a lower-dose statin, with a plan to uptitrate depending on each patients’ response to treatment.
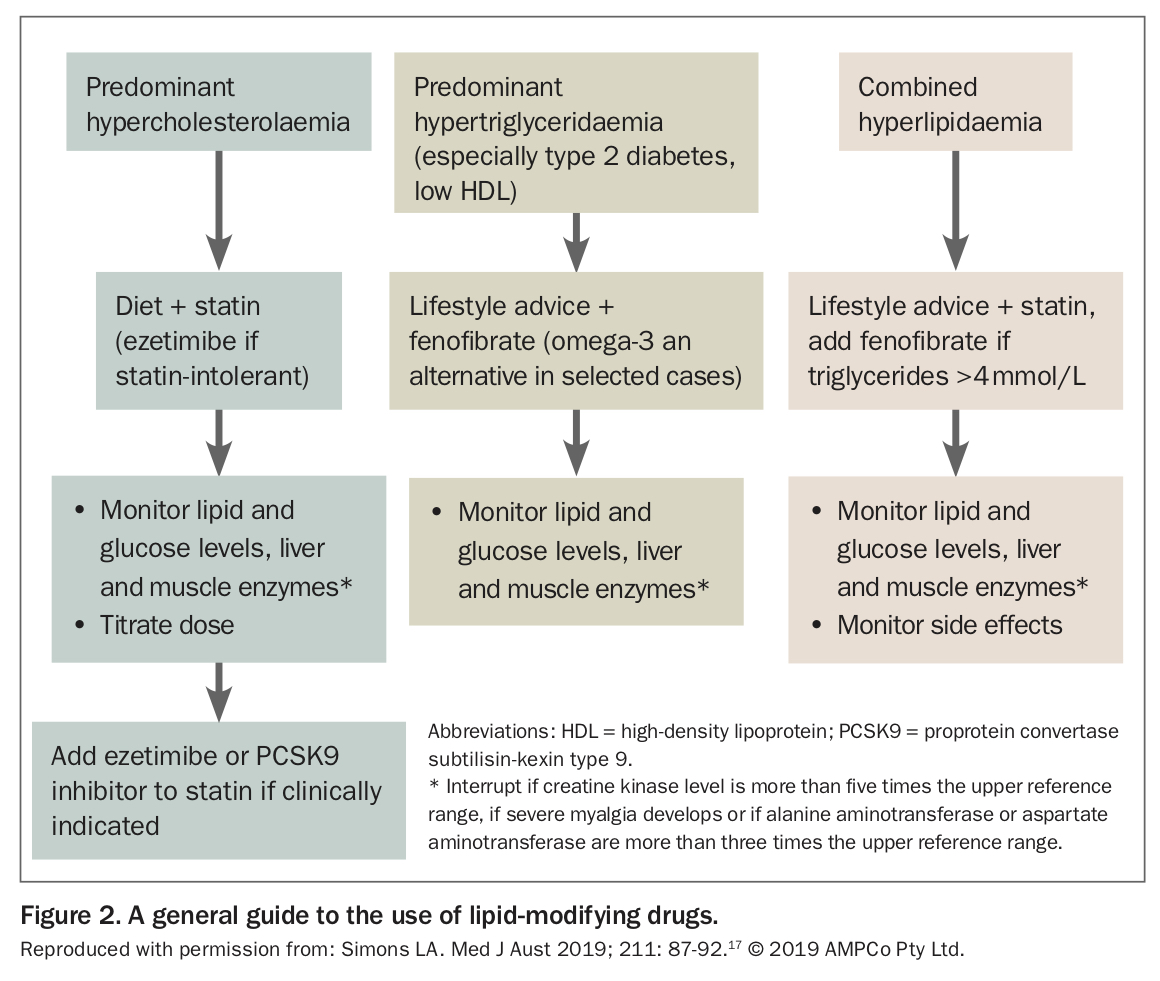
In general practice, the selection of appropriate lipid-lowering therapy, after diet and lifestyle advice, is still determined by identification of the predominant lipid pattern present. Does this patient have predominant hypercholesterolaemia or predominant hypertriglyceridaemia or combined hyperlipidaemia? A general guide to the selection of lipid-modifying drugs is presented in Figure 2.
{kind=link}
Conclusion
Lipid-modifying therapy reduces CVD risk in many patients, especially in those with pre-existing CVD. There remains a large unmet need for better CVD prevention via lipid control, with many patients not receiving lipid-lowering therapy according to guidelines. In addition to statins and ezetimibe, PCSK9 inhibitors offer additional CVD prevention. The guidance underlying lipid management is clear: intensive lipid-lowering therapy is required in secondary prevention; less intensive therapy, applied selectively, is required in primary prevention. CT
COMPETING INTERESTS: Associate Professor Simons has previously received clinical trial or consultancy fees from manufacturers of lipid-modifying drugs.