Heart transplantation: care of recipients

GPs do not commonly see patients who have undergone heart transplantation, although the number of recipients each year is increasing. Prompt contact with the transplant centre for specialised review by the heart transplant team is recommended in the event of a patient exhibiting early signs of complications.
- Care for heart transplant recipients encompasses a wide range of complex medical problems and requires the primary treating clinician to be highly vigilant of the possible complications that may arise, including infection, malignancy, hypertension and diabetes.
- A patient with allograft rejection may exhibit symptoms such as dyspnoea and palpitations and present with signs of fluid retention. At times they may be asymptomatic or present with nonspecific symptoms such as fatigue. A screening echocardiogram is appropriate until an endomyocardial biopsy can be performed in a transplant centre.
- To prevent rejection, monitoring of trough calcineurin inhibitor and proliferation signalling inhibitor levels, which may be affected by some foods and medications, is important. Long-term adjustment of levels is best performed in transplant centres during regular review.
- Prompt contact with the transplant centre for specialised review by the heart transplant team is recommended in the event of a patient exhibiting early signs of complications.
Heart transplantation has evolved over the past 50 years and is now incorporated into the treatment repertoire of advanced heart failure as the definitive management strategy for patients with disease that is refractory to other medical therapies. In Australia, 93 heart transplantations were performed in 2017, and numbers are gradually increasing each year.1
Heart transplant centres have been established in metropolitan areas in New South Wales, Victoria, Queensland and Western Australia. The overall survival rate after an orthotopic heart transplant is about 87.5% at one year, 80% at five years and 50% at 15 years.1 About 1400 heart transplant recipients live in Australia. Owing to geographical constraints, a significant proportion of these patients need to travel for several hours to be reviewed at the nearest heart transplant centre.1
Surgical technique and immediate postoperative care
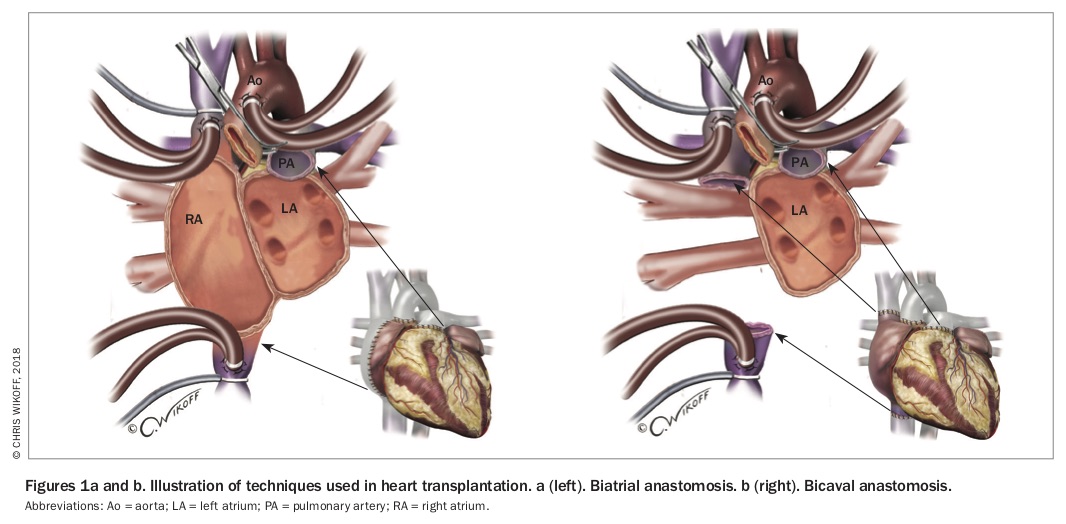
In a standard orthotopic heart transplant operation, the native heart is excised except for cuffs of the left and right atria. The donor heart is then anastamosed to the recipient at the level of the aorta, pulmonary artery and the left and right atria. The native pulmonary arteries are generally preserved with the residual left atrial tissue using a biatrial anastomosis technique (Figure 1a). Another technique, bicaval anastomosis, involves complete removal of the native right atrium (Figure 1b).2 The median hospital length of stay after heart transplantation is about two weeks.3
{kind=link}
Surveillance for allograft rejection
A significant proportion of recipients experience graft rejection at varying severity after transplantation, and up to 20% of patients require treatment for acute rejection.3 Endomyocardial biopsies of the interventricular septum for allograft rejection surveillance are routinely performed via central venous access in the first six to 12 months. The risk of acute rejection is inversely proportional to the time from transplantation, and the highest risk is within the first six months.4
Acute cellular allograft rejection is primarily driven by T cell-mediated responses, which can be reliably detected on microscopy of endomyocardial biopsy specimens before they manifest as a reduction of left ventricular function on echocardiogram.4 Antibody-mediated rejection is less common, and can be diagnosed through immunohistochemical staining of endomyocardial biopsy specimens as well as serological testing of donor-specific antibodies.4 Limitations of endomyocardial biopsy includes its invasiveness as a procedure and possible sampling error if the rejection process only affects the myocardium in a patchy nature. Newer techniques such as cardiac MRI have shown promise as a noninvasive alternative to endomyocardial biopsy.5
Patients with allograft rejection may exhibit symptoms such as dyspnoea and palpitations and present with signs of fluid retention. At times, patients may be asymptomatic or present with nonspecific symptoms such as fatigue. A screening echocardiogram would be appropriate until an endomyocardial biopsy can be performed in a transplant centre. In most instances, a tapering course of high-dose corticosteroids would result in complete resolution without long-term sequelae.4
Immunosuppression regimen
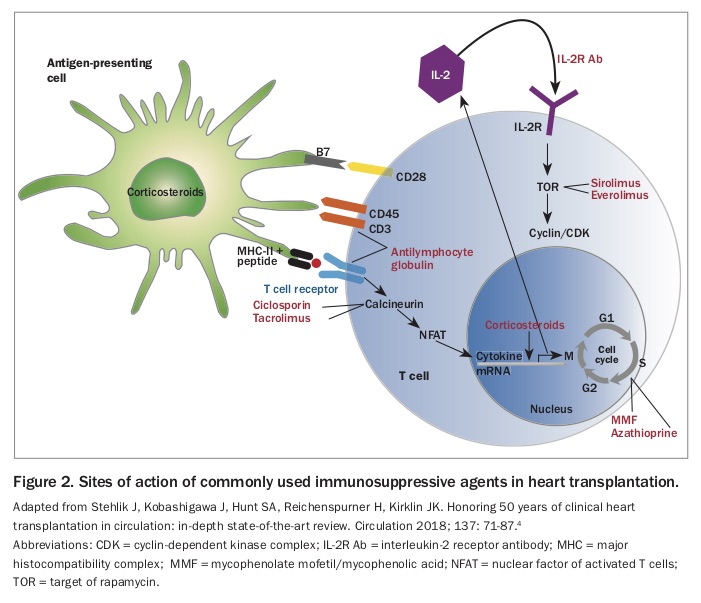
About 50% of heart transplant recipients receive induction immunosuppression at the time of transplantation with an interleukin-2 receptor antagonist basiliximab (off-label use) and, now to a lesser extent, T cell-depletion therapy using anti-thymocyte immunoglobulin (off-label use). The long-term immunosuppression regimen after heart transplantation comprises a calcineurin inhibitor (CNI; tacrolimus or ciclosporin), an antimetabolite (mycophenolate or azathioprine) and a corticosteroid.6 In recent years, the proliferation signalling inhibitors (PSIs) sirolimus and everolimus (also known as mechanistic target of rapamycin [mTOR] inhibitors) have been used increasingly due to the protection they provide against malignancy and coronary vasculopathy. As PSIs delay wound healing, they are not introduced until after surgical healing is complete.7 It should be noted that although they have renal preservation properties when used in place of CNIs, they could increase the concentration of CNI and worsen the renal toxicity when used in combination.7,8 The sites of action for these immunosuppressive therapies are shown in Figure 2.4
{kind=link}
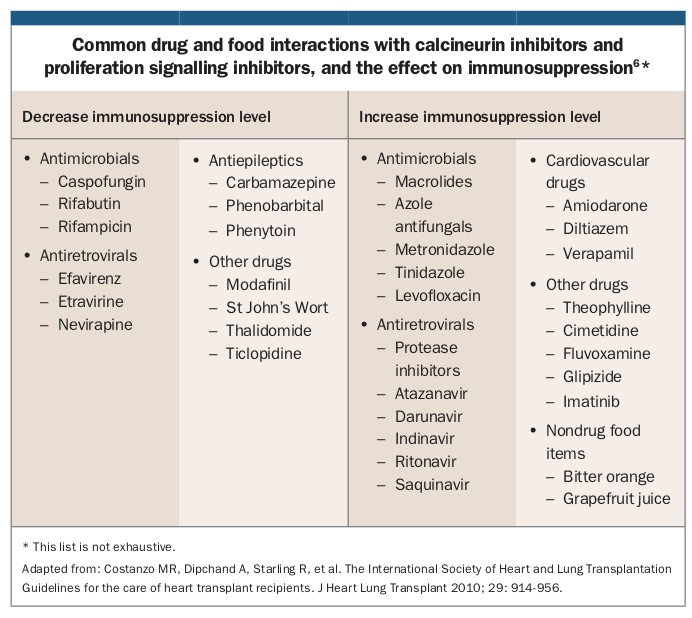
In low-risk patients who have a favourable rejection profile, corticosteroids can be safely weaned over the first six to 12 months after transplantation.6 Therapeutic monitoring of trough CNI and PSI levels is particularly important to prevent rejection. This is especially the case given the long list of drug interactions of these medications because they are metabolised by the cytochrome P450 pathway (CYP 3A4).6 Long-term adjustment of CNI and PSI levels is best performed in transplant centres during regular review. The Box lists some of medications and foods that may affect the plasma concentration of CNIs and PSIs.6
{kind=link}
Allograft vasculopathy
Cardiac allograft vasculopathy (CAV) affects about 10% of patients at one year, 30% at five years and 50% at 10 years.3 CAV manifests as a diffuse process that involves pan-arterial intimal thickening, rather than atherosclerotic plaques, which are associated with native coronary disease. The mechanism is thought to be chronic inflammation due to immune activation, but traditional risk factors may accelerate this process.4
Transplant patients with CAV usually present with atypical symptoms such as fatigue or decreased exercise tolerance. Due to the denervation of the heart during transplant, the ischaemic pain response is often blunted, making routine annual surveillance more important in identifying early disease.4,6 Invasive coronary angiography is the gold standard for assessment of CAV, but CT coronary angiography is an excellent noninvasive alternative surveillance method and has excellent sensitivity and specificity.3,9 However, due to the high prevalence of renal impairment among heart transplant recipients, yearly functional assessment with stress echocardiogram or nuclear myocardial perfusion scanning is suggested.3
Infection and malignancy
The major early causes of mortality within the first five years after transplantation are infection and rejection; and after five years, noncardiac causes, CAV and malignancy become the leading causes of death.1 Immunosuppression is gradually tapered after transplantation, but, unlike infection, the risk of malignancy is proportional to the duration rather than the level of immunosuppression.4
Infection accounts for almost one-third of mortality in the first year after heart transplantation, with the most common serious infections being bacterial pneumonia, invasive fungal infections and cytomegalovirus (CMV) reactivation.3,4 Therefore, antimicrobial therapies are used as prophylaxis, particularly in the early post-transplant period. For the first three to six months, patients typically receive systemic azole antifungal for fungal prophylaxis as well as oral valganciclovir for CMV prophylaxis if either the donor or recipient is CMV positive.6 A sulfamethoxazole and trimethoprim combination twice weekly is recommended for Pneumocystis jiroveci pneumonia and toxoplasmosis prophylaxis.4,6
All age-appropriate vaccinations including influenza vaccines are recommended for heart transplant recipients. The exceptions are live virus vaccines, which are contraindicated due to the risk of causing serious infection from the attenuated virus in the context of immunosuppression. Antibiotic prophylaxis for elective surgery and dental procedures is also recommended.4
Meticulous age-appropriate malignancy screening is essential after transplantation. All forms of malignancies combined account for more than one quarter of mortality five years or more after heart transplantation.1 Skin cancers comprise most cancers diagnosed after transplantation, and yearly skin checks are recommended, particularly for individuals who have the usual risk factors.4 Post-transplant lymphoproliferative disorder denotes a subtype of lymphoma seen only in transplant recipients. This condition may have an insidious onset and is often associated with Epstein-Barr virus reactivation.4
Hypertension, diabetes, renal dysfunction and osteoporosis
Long-term immunosuppression often leads to metabolic complications of hypertension and diabetes. Both of these conditions can contribute to renal dysfunction in addition to intrinsic CNI-related nephrotoxicity, necessitating close monitoring and optimisation of therapy.4 In addition, prolonged corticosteroid use leads to premature osteoporosis, which significantly increases fracture risk.3 Surveillance with bone mineral density testing and appropriate vitamin D replacement is instituted early after transplantation.
Hypertension treatment in heart transplant recipients should have the same goal as in the general population, particularly as these patients are more at risk of CAV. Diet and lifestyle modification should be first-line therapy. First-line pharmacotherapy often consists of calcium channel blockers, but an ACE inhibitor or an angiotensin receptor blocker would be preferred in patients with diabetes due to their renal protective effects.3
About 25% of patients have diabetes one year after transplantation, and this rises to 37% at five years.10 Poor glycaemic control can lead to increased mortality and morbidity. It is also of note that heart transplant patients may have atypical responses to hypoglycaemia due to cardiac denervation. In the early post-transplant period, insulin is the safest hypoglycaemic agent and is easily titratable to the dosages of corticosteroids used for immunosuppression.10 Oral hypoglycaemic agents should be used with caution and in consultation with specialised transplant endocrine centres. Although metformin is first-line therapy in the general population, its use in the heart transplant population carries increased risk of lactic acidosis during periods of acute renal injury or severe infection.10 Sodium-glucose cotransporter-2 inhibitors have shown promise due to their protective effects against adverse cardiovascular outcomes, but their use in the transplant population requires clarification through further research.10,11
Conclusion
Care for heart transplant recipients encompasses a wide range of complex medical problems and requires the primary treating clinician to be highly vigilant of the possible complications that may arise. Prompt contact with the transplant centre for specialised review by the heart transplant team is recommended in the event of a patient exhibiting early signs of complications. CT